

Diagnostic profiles and clinical characteristics of youth referred to a pediatric mood disorders clinic
- PMID: 24638051
- PMCID: PMC3960293
- DOI: 10.1097/01.pra.0000445251.20875.47
Diagnostic profiles and clinical characteristics of youth referred to a pediatric mood disorders clinic
Abstract
Objectives: This study examined the diagnostic profiles and clinical characteristics of youth (ages 6-18 years) referred for diagnostic evaluation to a pediatric mood disorders clinic that specializes in early-onset bipolar disorder.
Method: A total of 250 youth were prescreened in an initial telephone intake, and 73 participated in a full diagnostic evaluation. Trained psychologists administered the Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime Version (K-SADSPL) to the child and to at least one parent, and a child psychiatrist conducted a separate pharmacological evaluation. Evaluators then met with a larger clinical team for a consensus diagnosticconference.
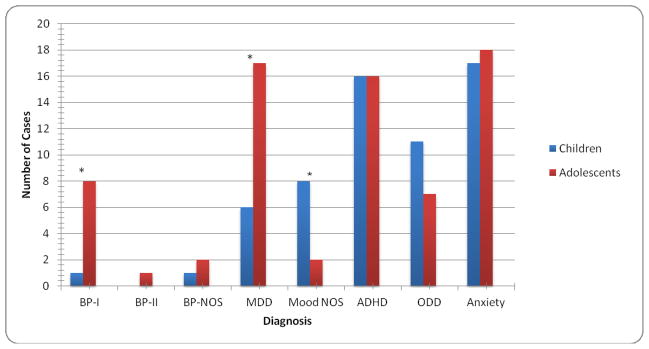
Results: Based on consensus diagnoses, 13 of the 73 referred youth (18%) met lifetime DSM-IV-TR criteria for a bipolar spectrum disorder (BSD; bipolar I, II or not otherwise specified disorder, or cyclothymic disorder). Of these 73, 27 (37%) were referred with a community diagnosis of a bipolar spectrum disorder, but only 7 of these 27 (26%) met DSM-IV-TR criteria for a bipolar spectrum diagnosis based on a structured interview and consensus diagnoses. The most common Axis I diagnoses (based on structured interview/consensus) were attentiondeficit/hyperactivity disorder (31/73, 42.5%) and major depressive disorder (23/73, 32%).
Conclusions: When youth referred for evaluation of BSD are diagnosed using standardized interviews with multiple reporters and consensus conferences, the "true positive" rate for bipolar spectrum diagnoses is relatively low. Reasons for the discrepancy between community and research-based diagnoses of pediatric BSD- including the tendency to stretch the BSD criteria to include children with depressive episodes and only 1-2 manic symptoms-are discussed.
Conflict of interest statement
All authors declare no conflicts of interest.
Figures
Similar articles
-
Occult mood disorders in 104 consecutively presenting children referred for the treatment of attention-deficit/hyperactivity disorder in a community mental health clinic.J Clin Psychiatry. 2003 Oct;64(10):1170-6; quiz, 1274-6. doi: 10.4088/jcp.v64n1005. J Clin Psychiatry. 2003. PMID: 14658964
-
Phenomenology of bipolar disorder not otherwise specified in youth: a comparison of clinical characteristics across the spectrum of manic symptoms.Bipolar Disord. 2013 May;15(3):240-52. doi: 10.1111/bdi.12054. Epub 2013 Mar 25. Bipolar Disord. 2013. PMID: 23521542 Free PMC article.
-
Borderline personality disorder characteristics in young adults with recurrent mood disorders: a comparison of bipolar and unipolar depression.J Affect Disord. 2005 Jul;87(1):17-23. doi: 10.1016/j.jad.2005.02.019. J Affect Disord. 2005. PMID: 15967232
-
Prepubertal and early adolescent bipolar I disorder: review of diagnostic validation by Robins and Guze criteria.J Clin Psychiatry. 2005;66 Suppl 7:21-8. J Clin Psychiatry. 2005. PMID: 16124838 Review.
-
ECNP consensus meeting. Bipolar depression. Nice, March 2007.Eur Neuropsychopharmacol. 2008 Jul;18(7):535-49. doi: 10.1016/j.euroneuro.2008.03.003. Epub 2008 May 23. Eur Neuropsychopharmacol. 2008. PMID: 18501566 Review.
Cited by
-
Distinguishing bipolar disorder from other psychiatric disorders in children.Curr Psychiatry Rep. 2014 Dec;16(12):516. doi: 10.1007/s11920-014-0516-2. Curr Psychiatry Rep. 2014. PMID: 25315116 Review.
-
Frontal alpha asymmetry predicts inhibitory processing in youth with attention deficit/hyperactivity disorder.Neuropsychologia. 2017 Jul 28;102:45-51. doi: 10.1016/j.neuropsychologia.2017.06.003. Epub 2017 Jun 3. Neuropsychologia. 2017. PMID: 28587767 Free PMC article.
-
Comparing the CASI-4R and the PGBI-10 M for Differentiating Bipolar Spectrum Disorders from Other Outpatient Diagnoses in Youth.J Abnorm Child Psychol. 2017 Apr;45(3):611-623. doi: 10.1007/s10802-016-0182-4. J Abnorm Child Psychol. 2017. PMID: 27364346 Free PMC article.
References
-
- Perlis RH, Miyahara S, Marangell LB, et al. Long-term implications of early onset in bipolar disorder: Data from the first 1000 participants in the systematic treatment enhancement program for bipolar disorder (STEP-BD) Biol Psychiatry. 2004;55(9):875–881. - PubMed
-
- Youngstrom E, Van Meter A, Algorta GP. The bipolar spectrum: myth or reality? Current Psychiatry Reports. 2010;12:479–489. - PubMed
-
- Moreno C, Laje G, Blanco C, et al. National trends in the outpatient diagnosis and treatment of bipolar disorder in youth. Arch Gen Psychiatry. 2007;64(9):1032–1039. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
