

Pulse oximetry for perioperative monitoring
- PMID: 24638894
- PMCID: PMC6464860
- DOI: 10.1002/14651858.CD002013.pub3
Pulse oximetry for perioperative monitoring
Abstract
Background: This is an update of a review last published in Issue 9, 2009, of The Cochrane Library. Pulse oximetry is used extensively in the perioperative period and might improve patient outcomes by enabling early diagnosis and, consequently, correction of perioperative events that might cause postoperative complications or even death. Only a few randomized clinical trials of pulse oximetry during anaesthesia and in the recovery room have been performed that describe perioperative hypoxaemic events, postoperative cardiopulmonary complications and cognitive dysfunction.
Objectives: To study the use of perioperative monitoring with pulse oximetry to clearly identify adverse outcomes that might be prevented or improved by its use.The following hypotheses were tested.1. Use of pulse oximetry is associated with improvement in the detection and treatment of hypoxaemia.2. Early detection and treatment of hypoxaemia reduce morbidity and mortality in the perioperative period.3. Use of pulse oximetry per se reduces morbidity and mortality in the perioperative period.4. Use of pulse oximetry reduces unplanned respiratory admissions to the intensive care unit (ICU), decreases the length of ICU readmission or both.
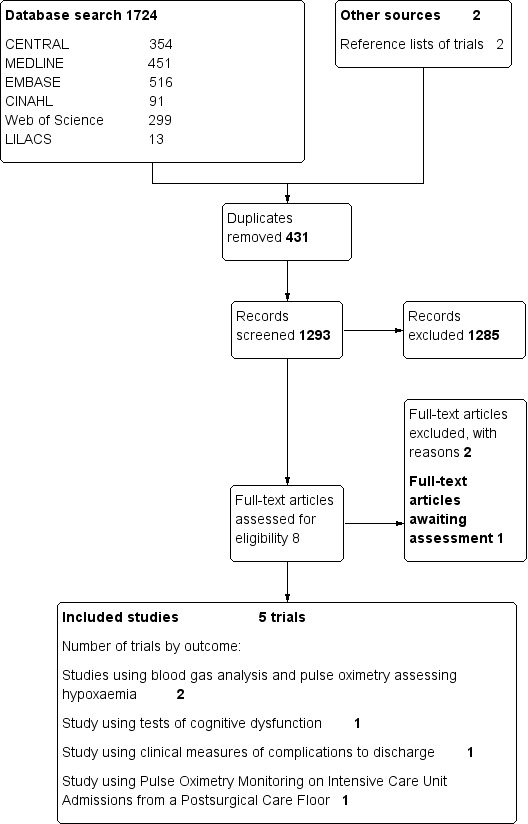
Search methods: We searched the Cochrane Central Register of Controlled Trials (CENTRAL) (2013, Issue 5), MEDLINE (1966 to June 2013), EMBASE (1980 to June 2013), CINAHL (1982 to June 2013), ISI Web of Science (1956 to June 2013), LILACS (1982 to June 2013) and databases of ongoing trials; we also checked the reference lists of trials and review articles. The original search was performed in January 2005, and a previous update was performed in May 2009.
Selection criteria: We included all controlled trials that randomly assigned participants to pulse oximetry or no pulse oximetry during the perioperative period.
Data collection and analysis: Two review authors independently assessed data in relation to events detectable by pulse oximetry, any serious complications that occurred during anaesthesia or in the postoperative period and intraoperative or postoperative mortality.
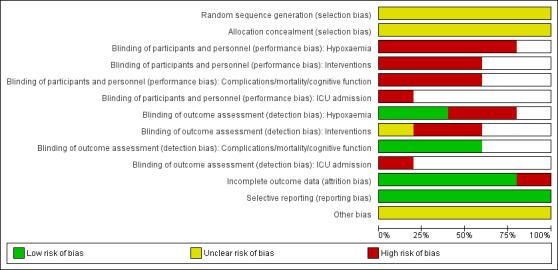
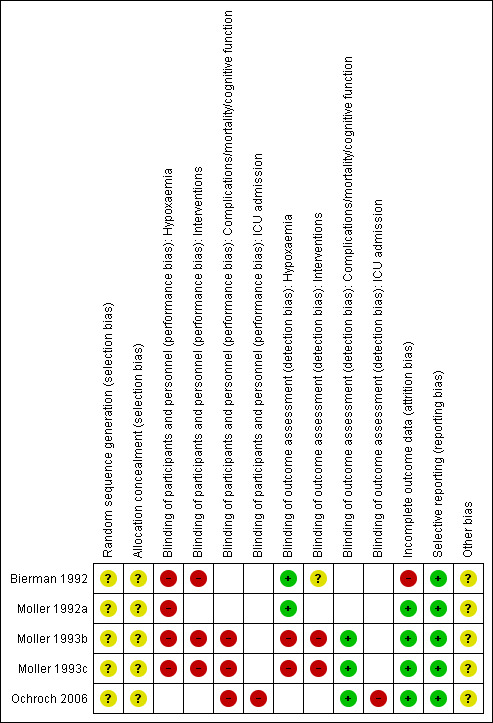
Main results: The last update of the review identified five eligible studies. The updated search found one study that is awaiting assessment but no additional eligible studies. We considered studies with data from a total of 22,992 participants that were eligible for analysis. These studies gave insufficient detail on the methods used for randomization and allocation concealment. It was impossible for study personnel to be blinded to participant allocation in the study, as they needed to be able to respond to oximetry readings. Appropriate steps were taken to minimize detection bias for hypoxaemia and complication outcomes. Results indicated that hypoxaemia was reduced in the pulse oximetry group, both in the operating theatre and in the recovery room. During observation in the recovery room, the incidence of hypoxaemia in the pulse oximetry group was 1.5 to three times less. Postoperative cognitive function was independent of perioperative monitoring with pulse oximetry. A single study in general surgery showed that postoperative complications occurred in 10% of participants in the oximetry group and in 9.4% of those in the control group. No statistically significant differences in cardiovascular, respiratory, neurological or infectious complications were detected in the two groups. The duration of hospital stay was a median of five days in both groups, and equal numbers of in-hospital deaths were reported in the two groups. Continuous pulse oximetry has the potential to increase vigilance and decrease pulmonary complications after cardiothoracic surgery; however, routine continuous monitoring did not reduce transfer to an ICU and did not decrease overall mortality.
Authors' conclusions: These studies confirmed that pulse oximetry can detect hypoxaemia and related events. However, we found no evidence that pulse oximetry affects the outcome of anaesthesia for patients. The conflicting subjective and objective study results, despite an intense methodical collection of data from a relatively large general surgery population, indicate that the value of perioperative monitoring with pulse oximetry is questionable in relation to improved reliable outcomes, effectiveness and efficiency. Routine continuous pulse oximetry monitoring did not reduce transfer to the ICU and did not decrease mortality, and it is unclear whether any real benefit was derived from the application of this technology for patients recovering from cardiothoracic surgery in a general care area.
Conflict of interest statement
Tom Pedesen is a co‐author of one study included in the review (Moller 1993c).
Amanda Nicholson: From March to August 2011, AN worked for the Cardiff Research Consortium, which provided research and consultancy services to the pharmaceutical industry. The Cardiff Research Consortium has no connection with AN's work with The Cochrane Collaboration. AN's husband has small direct holdings in several drug and biotech companies as part of a wider balanced share portfolio. See Sources of support.
Karen Hovhannisyan: none known.
Ann Merete Møller: none known.
Andrew F Smith: none known.
Sharon R Lewis: none known.
Figures
Update of
-
Pulse oximetry for perioperative monitoring.Cochrane Database Syst Rev. 2009 Oct 7;(4):CD002013. doi: 10.1002/14651858.CD002013.pub2. Cochrane Database Syst Rev. 2009. Update in: Cochrane Database Syst Rev. 2014 Mar 17;(3):CD002013. doi: 10.1002/14651858.CD002013.pub3. PMID: 19821289 Updated.
References
References to studies included in this review
Bierman 1992 {published data only}
-
- Bierman MI, Stein KL, Snyder JV. Pulse oximetry in the postoperative care of cardiac surgical patients. Chest 1992;102:1367‐70. [PUBMED: 1424853] - PubMed
Moller 1992a {published data only}
-
- Moller JT, Jensen PF, Johannessen NW, Espersen K. Hypoxaemia is reduced by pulse oximetry monitoring in the operating theatre and in the recovery room. British Journal of Anaesthesia 1992;68(2):146‐50. [PUBMED: 1540455] - PubMed
Moller 1993b {published data only}
-
- Moller JT, Svennild I, Johannessen NW. Perioperative monitoring with pulse oximetry and late postoperative cognitive dysfunction. British Journal of Anaesthesia 1993;71(3):340‐7. [PUBMED: 8398512] - PubMed
Moller 1993c {published data only}
-
- Moller JT, Johannessen NW, Espersen K, Ravlo O, Pedersen BD, Jensen PF, et al. Randomized evaluation of pulse oximetry in 20,802 patients: II. Perioperative events and postoperative complications. Anesthesiology 1993;78(3):445‐53. [PUBMED: 8457045] - PubMed
-
- Moller JT, Pedersen T, Rasmussen LS, Jensen PF, Pedersen BD, Ravlo O, et al. Randomized evaluation of pulse oximetry in 20,802 patients: I. Design, demography, pulse oximetry failure rate, and overall complication rate. Anesthesiology 1993;78(3):436‐44. [PUBMED: 8457044] - PubMed
Ochroch 2006 {published data only}
-
- Ochroch EA, Russell MW, Hanson WC 3rd, Devine GA, Cucchiara AJ, Weiner MG, et al. The impact of continuous pulse oximetry monitoring on intensive care unit admissions from a postsurgical care floor. Anesthesia and Analgesia 2006;102(3):868‐75. [PUBMED: 16492843] - PubMed
References to studies excluded from this review
Cullen 1992 {published data only}
-
- Cullen DJ, Nemeskal AR, Cooper JB, Zaslavsky A, Dwyer MJ. Effect of pulse oximetry, age, and ASA physical status on the frequency of patients admitted unexpectedly to a postoperative intensive care unit and the severity of their anesthesia‐related complications. Anesthesia and Analgesia 1992;74:177‐80. [PUBMED: 1731535] - PubMed
Mateer 1993 {published data only}
-
- Mateer JR, Olson DW, Stueven HA, Aufderheide TP. Continuous pulse oximetry during emergency endotracheal intubation. Annals of Emergency Medicine 1993;22:675‐9. [PUBMED: 8457094] - PubMed
References to studies awaiting assessment
Haines 2012 {published data only}
-
- Haines KL, Downs JB, Mullen MB, Klonsky JA, Gallagher SF. Scheduled, Intermittent oximetry fails to detect postoperative hypoxemia after bariatric surgery. Journal of Surgical Research 2012;172(2):287. [EMBASE: 70651408]
Additional references
Bendixen 1963
-
- Bendixen HH, Hedley‐Whyte J, Laver MB. Impaired oxygenation in surgical patients during general anaesthesia with controlled ventilation. New England Journal of Medicine 1963;269:991‐6. [PUBMED: 14059732] - PubMed
Canet 1991
-
- Canet J, Ricos M, Vidal F. Postanesthetic hypoxemia and oxygen administration. Anesthesiolgy 1991;74:1161‐2. [PUBMED: 2042775] - PubMed
Caplan 1990
-
- Caplan RA, Posner KL, Ward RJ, Cheney FW. Adverse respiratory events in anesthesia: a closed claim analysis. Anesthesiology 1990;72:828‐33. [PUBMED: 2339799] - PubMed
Cooper 1984
-
- Cooper JB, Newbower RS, Kitz RJ. An analysis of major errors and equipment failures in anesthesia management: considerations for prevention and detection. Anesthesiology 1984;60:34‐42. [PUBMED: 6691595 ] - PubMed
Cooper 1987
-
- Cooper JB, Cullen DJ, Nemeskal R, Hoaglin DC, Gevirtz CC, Csete M, et al. Effects of information feedback and pulse oximetry on incidence of anesthesia complications. Anesthesiology 1987;67:686‐94. [PUBMED: 3674468] - PubMed
Cote 1988
-
- Cote CJ, Goldstein EA, Cote MA, Hoaglin DC, Ryan JF. A single‐blind study of pulse oximetry in children. Anesthesiology 1988;68:184‐8. [PUBMED: 3277484] - PubMed
Cote 1991
-
- Cote CJ, Rolf N, Liu LM, Goudsouzian NG, Ryan JF, Zaslavsky A, et al. A single‐blind study of combined pulse oximetry and capnography in children. Anesthesiology 1991;74:980‐7. [PUBMED: 1904206] - PubMed
Guyatt 2008
Higgins 2011
Krasheninnikoff 1993
-
- Krasheninnikoff M, Ellitsgaard N, Rude C, Moller JT. Hypoxaemia after osteosynthesis of hip fractures. International Orthopaedics 1993;17(1):27‐9. [PUBMED: 8449619 ] - PubMed
Laver 1964
-
- Laver MB, Morgan J, Bendixen HH, Radford EP. Lung volume, compliance, and arterial oxygen tensions during controlled ventilation. Journal of Applied Physiology 1964;19:725‐33. [PUBMED: 14195585] - PubMed
Mlinaric 1997
-
- Mlinaric J, Nincevic N, Kostov D, Gnjatovic D. Pulse oximetry and capnometry in the prevention of perioperative morbidity and mortality. Lijecnicki Vjesnik 1997;119:113‐6. [PUBMED: 9490372] - PubMed
Moller 1998
-
- Moller JT, Cluitmans P, Rasmussen LS, Houx P, Rasmussen H, Canet J, et al. Long‐term postoperative cognitive dysfunction in the elderly ISPOCD1 study. ISPOCD Investigators. International Study of Post‐Operative Cognitive Dysfunction. Lancet 1998;351:857‐61. [PUBMED: 9525362] - PubMed
Møller 1994
-
- Møller JT. Anesthesia related hypoxemia. The effect of pulse oximetry monitoring on perioperative events and postoperative complications. Danish Medical Bulletin 1994;41(5):489‐500. [PUBMED: 7859517 ] - PubMed
Nunn 1965
-
- Nunn JF, Bergman NA, Coleman AJ, Jones DD. Factors influencing the arterial oxygen tension during anaesthesia with artificial ventilation. British Journal of Anaesthesia 1965;37:898‐914. - PubMed
Pedersen 1994
-
- Pedersen T. Complications and death following anaesthesia. A prospective study with special reference to the influence of patient‐, anaesthesia‐, and surgery‐related risk factors. Danish Medical Bulletin 1994;41(3):319‐31. [PUBMED: 7924461] - PubMed
RevMan 5.2 [Computer program]
-
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.2. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2012.
Rheineck 1996
-
- Rheineck‐Leyssius AT, Kalkman CJ, Trouwborst A. Influence of motivation of care providers on the incidence of postoperative hypoxaemia in the recovery room. British Journal of Anaesthesia 1996;77:453‐7. [PUBMED: : 8942327] - PubMed
Severinghaus 1992
-
- Severinghaus JW, Kelleher JF. Recent developments in pulse oximetry. Anesthesiology 1992;76:1018‐38. [PUBMED: 1599088] - PubMed
Shah 2013
-
- Shah A, Shelley KH. Is pulse oximetry an essential tool or just another distraction? The role of the pulse oximeter in modern anesthesia care. Journal of Clinical Monitoring and Computing 2013;27(3):235‐42. [PUBMED: 23314807] - PubMed
Stausholm 1997
-
- Stausholm K, Rosenberg‐Adamsen S, Edvardsen L, Kehlet H, Rosenberg J. Validation of pulse oximetry for monitoring of hypoxaemic episodes in the late postoperative period. British Journal of Anaesthesia 1997;78:86‐7. [PUBMED: 9059211 ] - PubMed
Tinker 1989
-
- Tinker JH, Dull DL, Caplan RA, Ward RJ, Cheney FW. Role of monitoring devices in preventing of anesthetic mishaps: a closed claims analysis. Anesthesiology 1989;71:541‐6. [PUBMED: 2508510] - PubMed
Townes 1989
-
- Townes BD, Bashein G, Hornbein TF, Coppel DB, Goldstein DE, Davis KB, et al. Neurobehavioral outcomes in cardiac operations. Journal of Thoracic and Cardiovascular Surgery 1989;98:774‐82. [PUBMED: 2811413] - PubMed
References to other published versions of this review
Pedersen 2003a
Pedersen 2003b
-
- Pedersen T, Dyrlund Pedersen B, Møller AM. Pulse oximetry for perioperative monitoring: systematic review of randomized trials. Anesthesia and Analgesia 2003;96:426‐31. [PUBMED: 12917918 ] - PubMed
Pedersen 2003c
-
- Poulsen A, Pedersen T. Pulse oximetry in perioperative monitoring. Ugeskrift for Laeger 2003;165(42):4025‐7. [PUBMED: 14610837] - PubMed
Pedersen 2005
-
- Pedersen T. Does perioperative pulse oximetry improve outcome? Seeking the best available evidence to answer the clinical question. Best Practice and Research. Clinical Anaesthesiology 2005;19(1):111‐23. [PUBMED: 15679062 ] - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical