

Cohort Profile: The Malawi Longitudinal Study of Families and Health (MLSFH)
- PMID: 24639448
- PMCID: PMC4469793
- DOI: 10.1093/ije/dyu049
Cohort Profile: The Malawi Longitudinal Study of Families and Health (MLSFH)
Abstract
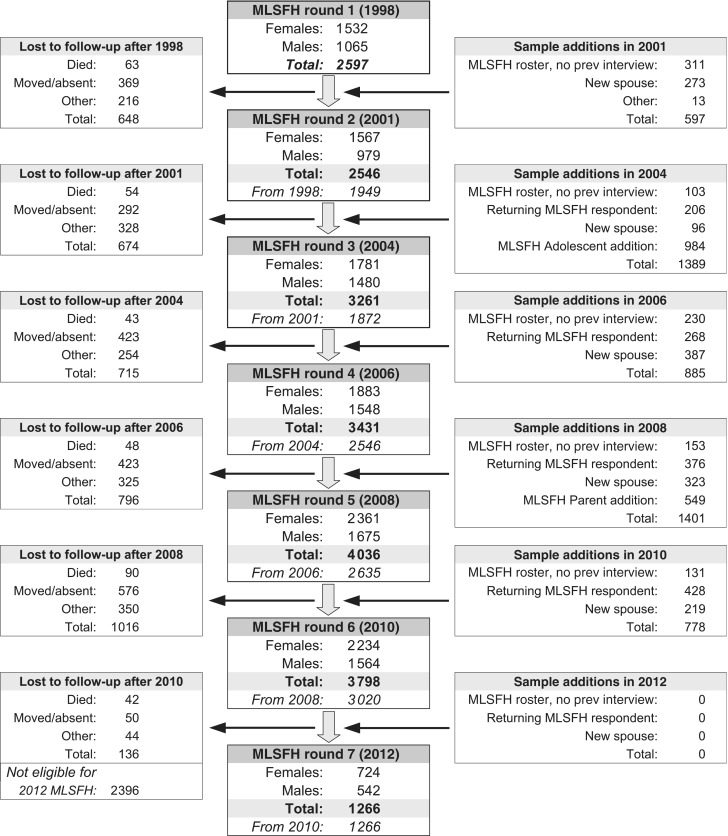
The Malawi Longitudinal Study of Families and Health (MLSFH) is one of very few long-standing, publicly available longitudinal cohort studies in a sub-Saharan African (SSA) context. It provides a rare record of more than a decade of demographic, socioeconomic and health conditions in one of the world's poorest countries. The MLSFH was initially established in 1998 to study social network influences on fertility behaviours and HIV risk perceptions, and over time the focus of the study expanded to include health, sexual behaviours, intergenerational relations and family/household dynamics. The currently available data include MLSFH rounds collected in 1998, 2001, 2004, 2006, 2008, 2010 and 2012 for up to 4000 individuals, providing information about socioeconomic and demographic characteristics, sexual behaviours, marriage, household/family structure, risk perceptions, social networks and social capital, intergenerational relations, HIV/AIDS and other dimensions of health. The MLSFH public use data can be requested on the project website: http://www.malawi.pop.upenn.edu/.
© The Author 2014; all rights reserved. Published by Oxford University Press on behalf of the International Epidemiological Association.
Figures

References
-
- Gootjes J, Tel RM, Bergkamp FJM, Gorgels JPMC. Laboratory evaluation of a novel capillary blood sampling device for measuring eight clinical chemistry parameters and HbA1c. Clin Chim Acta 2009;401:152–57. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01 HD053781/HD/NICHD NIH HHS/United States
- R03 HD058976/HD/NICHD NIH HHS/United States
- R01 HD044228/HD/NICHD NIH HHS/United States
- P30 AI045008/AI/NIAID NIH HHS/United States
- NIAID AI045008/PHS HHS/United States
- R01 HD041713/HD/NICHD NIH HHS/United States
- R24 HD044964/HD/NICHD NIH HHS/United States
- R01 HD37276/HD/NICHD NIH HHS/United States
- R01 HD/MH041713/HD/NICHD NIH HHS/United States
- NIA P30 AG12836/AG/NIA NIH HHS/United States
- P2C HD044964/HD/NICHD NIH HHS/United States
- NICHD R24 HD044964/PHS HHS/United States
- R21 HD050652/HD/NICHD NIH HHS/United States
- R21 HD071471/HD/NICHD NIH HHS/United States
- NICHD R01HD053781/PHS HHS/United States
- R24 HD041022/HD/NICHD NIH HHS/United States
- NIAID AI 045008/PHS HHS/United States
- P30 AG012836/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
