

Rectourethral fistula: systemic review of and experiences with various surgical treatment methods
- PMID: 24639969
- PMCID: PMC3953168
- DOI: 10.3393/ac.2014.30.1.35
Rectourethral fistula: systemic review of and experiences with various surgical treatment methods
Abstract
Purpose: A rectourethral fistula (RUF) is an uncommon complication resulting from surgery, radiation or trauma. Although various surgical procedures for the treatment of an RUF have been described, none has gained acceptance as the procedure of choice. The aim of this study was to review our experience with surgical management of RUF.
Methods: The outcomes of 6 male patients (mean age, 51 years) with an RUF who were operated on by a single surgeon between May 2005 and July 2012 were assessed.
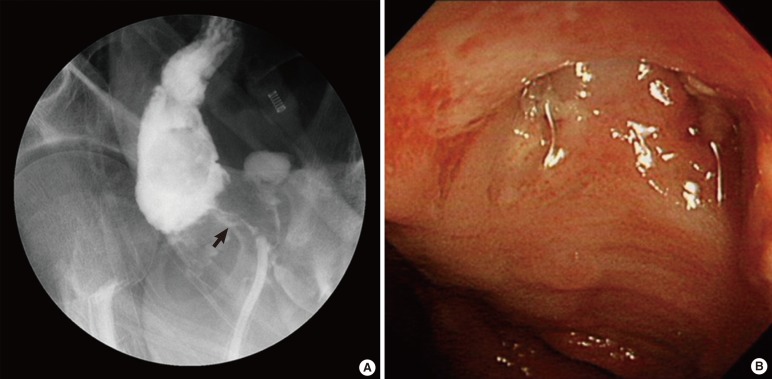
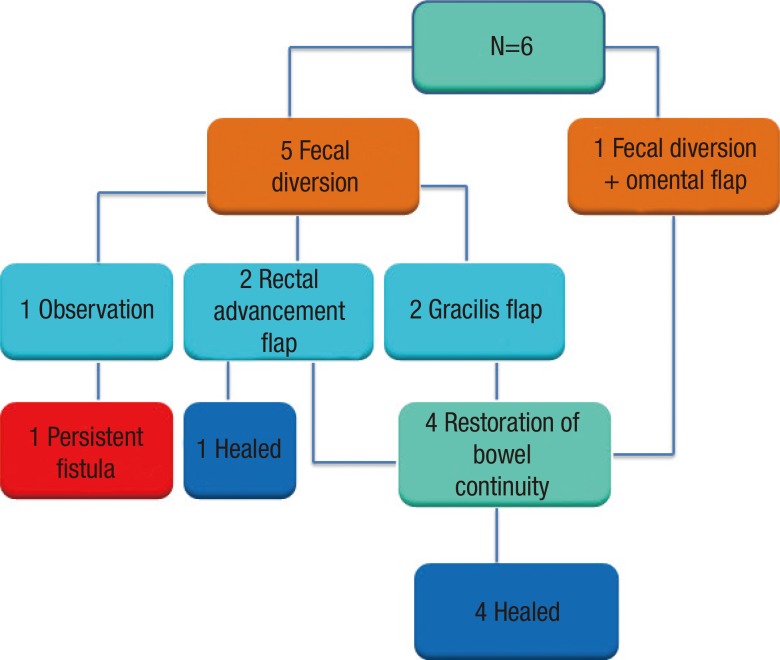
Results: The causes of the RUF were iatrogenic in four cases (two after radiation therapy for rectal cancer, one after brachytherapy for prostate cancer, and one after surgery for a bladder stone) and traumatic in two cases. Fecal diversion was the initial treatment in five patients. In one patient, fecal diversion was performed simultaneously with definitive repair. Four patients underwent staged repair after a mean of 12 months. Rectal advancement flaps were done for simple, small fistula (n = 2), and flap interpositions (gracilis muscle flap, n = 2; omental flap, n = 1) were done for complex or recurrent fistulae. Urinary strictures and incontinence were observed in patients after gracilis muscle flap interposition, but they were resolved with simple treatments. The mean follow-up period was 28 months, and closure of the fistula was achieved in all five patients (100%) who underwent definitive repairs. The fistula persisted in one patient who refused further definitive surgery after receiving only a fecal diversion.
Conclusion: Depending on the severity and the recurrence status of RUF, a relatively simple rectal advancement flap repair or a more complex gracilis muscle or omental flap interposition can be used to achieve closure of the fistula.
Keywords: Complication; Rectal fistula; Surgical flap; Urinary fistula.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures


Similar articles
-
Gracilis muscle interposition flap repair of urinary fistulae: pelvic radiation is associated with persistent urinary incontinence and decreased quality of life.World J Urol. 2016 Jan;34(1):131-6. doi: 10.1007/s00345-015-1597-1. Epub 2015 May 26. World J Urol. 2016. PMID: 26008116
-
Rectourethral Fistula Induced by Localised Prostate Cancer Treatment: Surgical and Functional Outcomes of Transperineal Repair with Gracilis Muscle Flap Interposition.Eur Urol. 2022 Mar;81(3):305-312. doi: 10.1016/j.eururo.2021.09.017. Epub 2021 Oct 20. Eur Urol. 2022. PMID: 34686386
-
Preventing Rectourethral Fistula Recurrence With Gracilis Flap.Ann Plast Surg. 2022 May 1;88(4 Suppl 4):S316-S319. doi: 10.1097/SAP.0000000000003085. Epub 2022 Feb 21. Ann Plast Surg. 2022. PMID: 35180755
-
Acquired Rectourethral and Rectovaginal Fistulas in Children: A Systematic Review.Front Pediatr. 2021 May 7;9:657251. doi: 10.3389/fped.2021.657251. eCollection 2021. Front Pediatr. 2021. PMID: 34026691 Free PMC article.
-
Complications after radical prostatectomy: anastomotic stricture and rectourethral fistula.Curr Opin Urol. 2011 Nov;21(6):461-4. doi: 10.1097/MOU.0b013e32834b7e1b. Curr Opin Urol. 2011. PMID: 21934623 Review.
Cited by
-
Rectourethral fistula.Ann Gastroenterol. 2019 Mar-Apr;32(2):212. doi: 10.20524/aog.2018.0335. Epub 2018 Dec 7. Ann Gastroenterol. 2019. PMID: 30872914 Free PMC article. No abstract available.
-
A rare case of tubercular recto-prostatic urethral fistula with tuberculous orchitis.Urol Case Rep. 2020 Jul 27;33:101355. doi: 10.1016/j.eucr.2020.101355. eCollection 2020 Nov. Urol Case Rep. 2020. PMID: 33102054 Free PMC article.
-
A rare case of fatal rectal perforation and sepsis following traumatic urinary catheterization.Urol Case Rep. 2024 Mar 12;54:102706. doi: 10.1016/j.eucr.2024.102706. eCollection 2024 May. Urol Case Rep. 2024. PMID: 38827535 Free PMC article.
-
Clinical outcome and quality of life after gracilis muscle transposition for fistula closure over a 10-year period.Int J Colorectal Dis. 2021 Mar;36(3):569-580. doi: 10.1007/s00384-020-03825-2. Epub 2021 Jan 2. Int J Colorectal Dis. 2021. PMID: 33386945
-
Transperineal approach to complex rectourinary fistulae.Can Urol Assoc J. 2015 Nov-Dec;9(11-12):E916-20. doi: 10.5489/cuaj.3107. Epub 2015 Dec 14. Can Urol Assoc J. 2015. PMID: 26788240 Free PMC article.
References
-
- Nyam DC, Pemberton JH. Management of iatrogenic rectourethral fistula. Dis Colon Rectum. 1999;42:994–997. - PubMed
-
- Hechenbleikner EM, Buckley JC, Wick EC. Acquired rectourethral fistulas in adults: a systematic review of surgical repair techniques and outcomes. Dis Colon Rectum. 2013;56:374–383. - PubMed
-
- Bukowski TP, Chakrabarty A, Powell IJ, Frontera R, Perlmutter AD, Montie JE. Acquired rectourethral fistula: methods of repair. J Urol. 1995;153(3 Pt 1):730–733. - PubMed
-
- Muñoz M, Nelson H, Harrington J, Tsiotos G, Devine R, Engen D. Management of acquired rectourinary fistulas: outcome according to cause. Dis Colon Rectum. 1998;41:1230–1238. - PubMed
-
- Parks AG, Motson RW. Peranal repair of rectoprostatic fistula. Br J Surg. 1983;70:725–726. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
