

Combat trauma-associated invasive fungal wound infections: epidemiology and clinical classification
- PMID: 24642013
- PMCID: PMC4946850
- DOI: 10.1017/S095026881400051X
Combat trauma-associated invasive fungal wound infections: epidemiology and clinical classification
Abstract
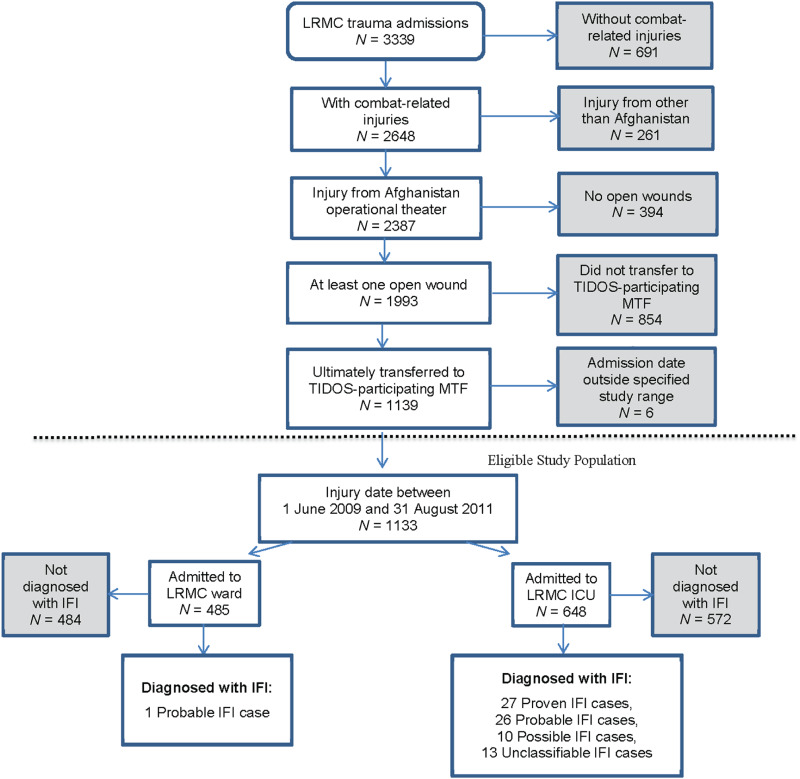
The emergence of invasive fungal wound infections (IFIs) in combat casualties led to development of a combat trauma-specific IFI case definition and classification. Prospective data were collected from 1133 US military personnel injured in Afghanistan (June 2009-August 2011). The IFI rates ranged from 0·2% to 11·7% among ward and intensive care unit admissions, respectively (6·8% overall). Seventy-seven IFI cases were classified as proven/probable (n = 54) and possible/unclassifiable (n = 23) and compared in a case-case analysis. There was no difference in clinical characteristics between the proven/probable and possible/unclassifiable cases. Possible IFI cases had shorter time to diagnosis (P = 0·02) and initiation of antifungal therapy (P = 0·05) and fewer operative visits (P = 0·002) compared to proven/probable cases, but clinical outcomes were similar between the groups. Although the trauma-related IFI classification scheme did not provide prognostic information, it is an effective tool for clinical and epidemiological surveillance and research.
Conflict of interest statement
None.
Figures
References
-
- Eucker J, et al. Mucormycoses. Mycoses 2001; 44: 253–260. - PubMed
-
- Lanternier F, et al. A global analysis of mucormycosis in France: the RetroZygo Study (2005–2007). Clinical Infectious Diseases 2012; 54 (Suppl. 1): S35–S43. - PubMed
-
- Roden MM, et al. Epidemiology and outcome of zygomycosis: a review of 929 reported cases. Clinical Infectious Diseases 2005; 41: 634–653. - PubMed
-
- Steinbach WJ, et al. Clinical epidemiology of 960 patients with invasive aspergillosis from the PATH Alliance registry. Journal of Infection 2012; 65: 453–464. - PubMed
-
- Hajdu S, et al. Invasive mycoses following trauma. Injury 2009; 40: 548–554. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
