

Sympathetic activity-associated periodic repolarization dynamics predict mortality following myocardial infarction
- PMID: 24642467
- PMCID: PMC3973112
- DOI: 10.1172/JCI70085
Sympathetic activity-associated periodic repolarization dynamics predict mortality following myocardial infarction
Erratum in
- J Clin Invest. 2014 Jun 2;124(6):2808
Abstract
Background: Enhanced sympathetic activity at the ventricular myocardium can destabilize repolarization, increasing the risk of death. Sympathetic activity is known to cluster in low-frequency bursts; therefore, we hypothesized that sympathetic activity induces periodic low-frequency changes of repolarization. We developed a technique to assess the sympathetic effect on repolarization and identified periodic components in the low-frequency spectral range (≤0.1 Hz), which we termed periodic repolarization dynamics (PRD).
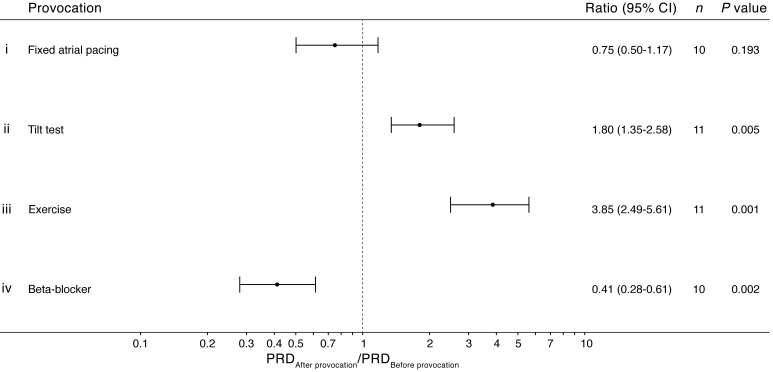
Methods: We investigated the physiological properties of PRD in multiple experimental studies, including a swine model of steady-state ventilation (n=7) and human studies involving fixed atrial pacing (n=10), passive head-up tilt testing (n=11), low-intensity exercise testing (n=11), and beta blockade (n=10). We tested the prognostic power of PRD in 908 survivors of acute myocardial infarction (MI). Finally, we tested the predictive values of PRD and T-wave alternans (TWA) in 2,965 patients undergoing clinically indicated exercise testing.
Results: PRD was not related to underlying respiratory activity (P<0.001) or heart-rate variability (P=0.002). Furthermore, PRD was enhanced by activation of the sympathetic nervous system, and pharmacological blockade of sympathetic nervous system activity suppressed PRD (P≤0.005 for both). Increased PRD was the strongest single risk predictor of 5-year total mortality (hazard ratio 4.75, 95% CI 2.94-7.66; P<0.001) after acute MI. In patients undergoing exercise testing, the predictive value of PRD was strong and complementary to that of TWA.
Conclusion: We have described and identified low-frequency rhythmic modulations of repolarization that are associated with sympathetic activity. Increased PRD can be used as a predictor of mortality in survivors of acute MI and patients undergoing exercise testing.
Trial registration: ClinicalTrials.gov NCT00196274.
Funding: This study was funded by Angewandte Klinische Forschung, University of Tübingen (252-1-0).
Figures




References
-
- Hunt SA, et al. 2009 focused update incorporated into the ACC/AHA 2005 Guidelines for the Diagnosis and Management of Heart Failure in Adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines: developed in collaboration with the International Society for Heart and Lung Transplantation. Circulation. 2009;119(14):e391–e479. doi: 10.1161/CIRCULATIONAHA.109.192065. - DOI - PubMed
-
- Task Force for Diagnosis and Treatment of Acute and Chronic Heart Failure 2008 of European Society of Cardiology, et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2008: the Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2008 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association of the ESC (HFA) and endorsed by the European Society of Intensive Care Medicine (ESICM). Eur Heart J. 2008;29(19):2388–2442. doi: 10.1093/eurheartj/ehn309. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
