

Tuberculosis among people living with HIV/AIDS in the German ClinSurv HIV Cohort: long-term incidence and risk factors
- PMID: 24646042
- PMCID: PMC3994660
- DOI: 10.1186/1471-2334-14-148
Tuberculosis among people living with HIV/AIDS in the German ClinSurv HIV Cohort: long-term incidence and risk factors
Abstract
Background: Tuberculosis (TB) still presents a leading cause of morbidity and mortality among people living with HIV/AIDS (PLWHA), including those on antiretroviral therapy. In this study, we aimed to determine the long-term incidence density rate (IDR) of TB and risk factors among PLWHA in relation to combination antiretroviral therapy (cART)-status.
Methods: Data of PLWHA enrolled from 2001 through 2011 in the German ClinSurv HIV Cohort were investigated using survival analysis and Cox regression.
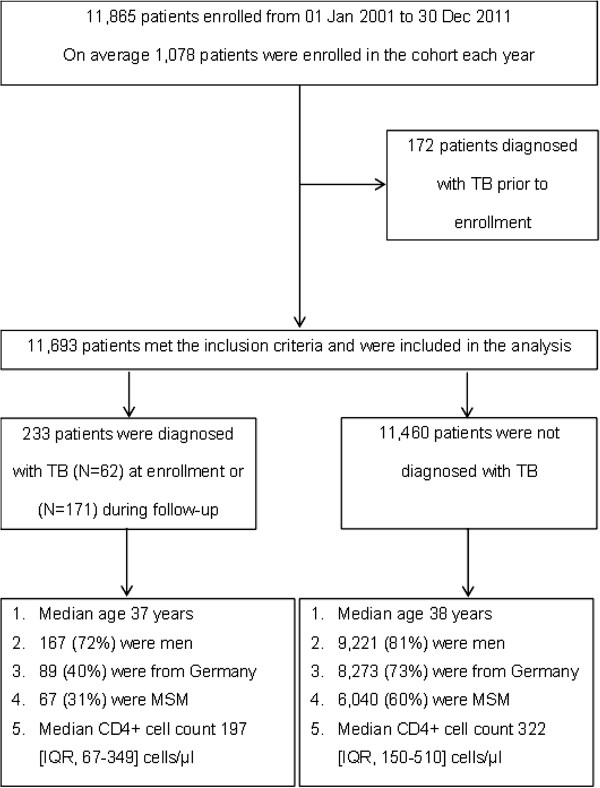
Results: TB was diagnosed in 233/11,693 PLWHA either at enrollment (N = 62) or during follow-up (N = 171). The TB IDR during follow-up was 0.37 cases per 100 person-years (PY) overall [95% CI, 0.32-0.43], and was higher among patients who never started cART and among patients originating from Sub-Saharan Africa (1.23 and 1.20 per 100PY, respectively). In two multivariable analyses, both patients (I) who never started cART and (II) those on cART shared the same risk factors for TB, namely: originating from Sub-Saharan Africa compared to Germany (I, hazard ratio (HR); [95% CI]) 4.05; [1.87-8.78] and II, HR 5.15 [2.76-9.60], CD4+ cell count <200 cells/μl (I, HR 8.22 [4.36-15.51] and II, HR 1.90 [1.14-3.15]) and viral load >5 log10 copies/ml (I, HR 2.51 [1.33-4.75] and II, HR 1.77 [1.11-2.82]). Gender, age or HIV-transmission risk group were not independently associated with TB.
Conclusion: In the German ClinSurv HIV cohort, patients originating from Sub-Saharan Africa, with low CD4+ cell count or high viral load at enrollment were at increased risk of TB even after cART initiation. As patients might be latently infected with Mycobacterium tuberculosis complex, early screening for latent TB infection and implementing isoniazid preventive therapy in line with available recommendations is crucial.
Figures


References
-
- World Health Organization. Global Tuberculosis Control 2012. Geneva: World Health Organization; 2012. Available at: http://apps.who.int/iris/bitstream/10665/75938/1/9789241564502_eng.pdf. Accessed 17 April 2013.
-
- Joint United Nations Programme on HIV/AIDS (UNAIDS) Global Report: UNAIDS Report on the Global AIDS Epidemic 2010. Geneva: UNAIDS; 2010. Available at: http://www.unaids.org/documents/20101123_globalreport_em.pdf. Accessed 25 March 2013.
-
- Grant AD, Bansi L, Ainsworth J, Anderson J, Delpech V, Easterbrook P, Fisher M, Gazzard B, Gilson R, Gompels M, Hill T, Johnson M, Leen C, Orkin C, Phillips AN, Porter K, Post F, Walsh J, Sabin CA. United Kingdom Collaborative HIV Cohort Study Group. Tuberculosis among people with HIV infection in the United Kingdom: opportunities for prevention? AIDS. 2009;14(18):2507–2515. - PubMed
-
- Haar CH, Cobelens FG, Kalisvaart NA, Van der Have JJ, Van Gerven PJ, Van Deutekom H. HIV prevalence among tuberculosis patients in The Netherlands, 1993–2001: trends and risk factors. Int J Tuberc Lung Dis. 2006;14(7):768–774. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
