

Variation in access to the liver transplant waiting list in the United States
- PMID: 24646768
- PMCID: PMC4211283
- DOI: 10.1097/01.TP.0000443223.89831.85
Variation in access to the liver transplant waiting list in the United States
Abstract
Background: We sought to compare liver transplant waiting list access by demographics and geography relative to the pool of potential liver transplant candidates across the United States using a novel metric of access to care, termed a liver wait-listing ratio (LWR).
Methods: We calculated LWRs from national liver transplant registration data and liver mortality data from the Scientific Registry of Transplant Recipients and the National Center for Healthcare Statistics from 1999 to 2006 to identify variation by diagnosis, demographics, geography, and era.
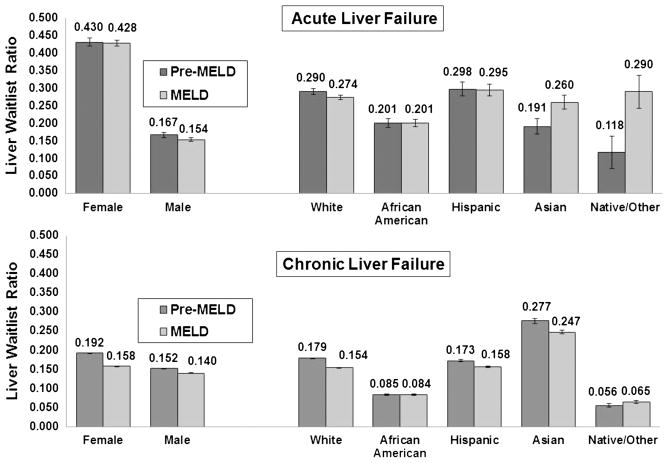
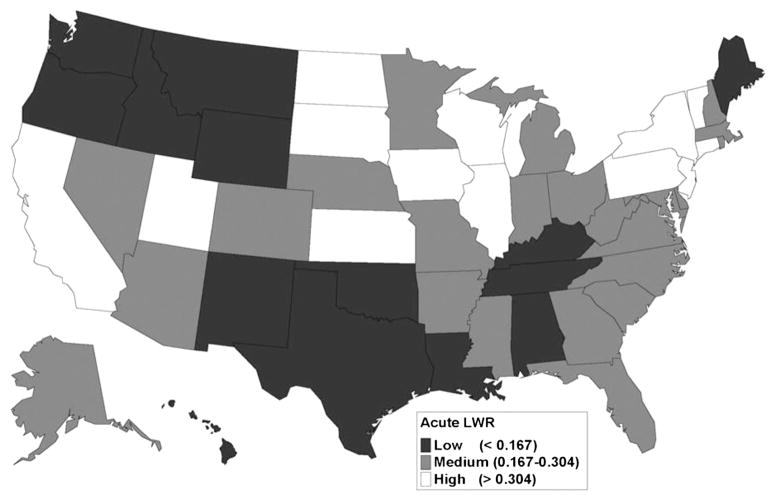
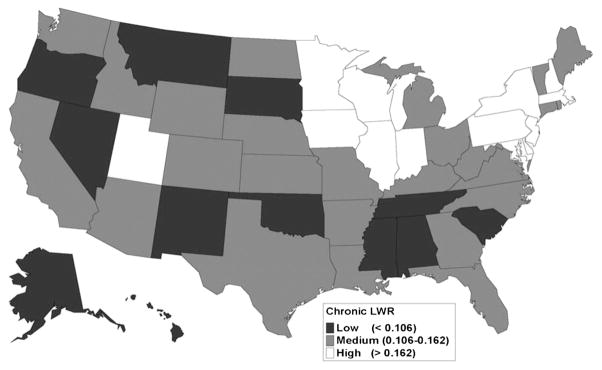
Results: Among patients with ALF and CLF, African Americans had significantly lower access to the waiting list compared with whites (acute: 0.201 versus 0.280; pre-MELD 0.201 versus 0.290; MELD era: 0.201 versus 0.274; all, P<0.0001) (chronic: 0.084 versus 0.163; pre-MELD 0.085 versus 0.179; MELD 0.084 versus 0.154; all, P<0.0001). Hispanics and whites had similar LWR in both eras (both P>0.05). In the MELD era, female subjects had greater access to the waiting list compared with male subjects (acute: 0.428 versus 0.154; chronic: 0.158 versus 0.140; all, P<0.0001). LWRs varied by three-fold by state (pre-MELD acute: 0.122-0.418, chronic: 0.092-0.247; MELD acute: 0.121-0.428, chronic: 0.092-0.243).
Conclusions: The marked inequity in early access to liver transplantation underscores the need for local and national policy initiatives to affect this disparity.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Thuluvath PJ, Guidinger MK, Fung JJ, et al. Liver transplantation in the United States, 1999–2008. Am J Transplant. 2010;10(4 Pt 2):1003. - PubMed
-
- Nguyen GC, Thuluvath PJ. Racial disparity in liver disease: biological, cultural, or socioeconomic factors. Hepatology. 2008;47:1058. - PubMed
-
- Kemmer N, Neff GW. Liver transplantation in the ethnic minority population: challenges and prospects. Dig Dis Sci. 2010;55:883. - PubMed
-
- Eckhoff DE, McGuire BM, Young CJ, et al. Race: a critical factor in organ donation, patient referral and selection, and orthotopic liver transplantation? Liver Transpl Surg. 1998;4:499. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
