

Optimal target localization for subthalamic stimulation in patients with Parkinson disease
- PMID: 24647024
- PMCID: PMC4001189
- DOI: 10.1212/WNL.0000000000000315
Optimal target localization for subthalamic stimulation in patients with Parkinson disease
Abstract
Objective: To further determine the causes of variable outcome from deep brain stimulation of the subthalamic nucleus (DBS-STN) in patients with Parkinson disease (PD).
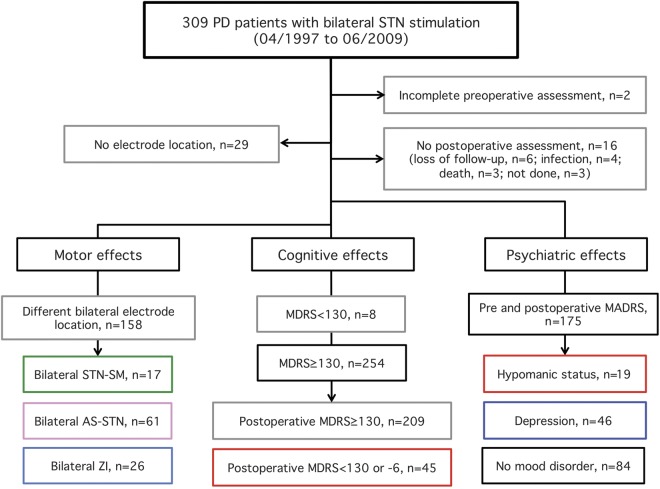
Methods: Data were obtained from our cohort of 309 patients with PD who underwent DBS-STN between 1996 and 2009. We examined the relationship between the 1-year motor, cognitive, and psychiatric outcomes and (1) preoperative PD clinical features, (2) MRI measures, (3) surgical procedure, and (4) locations of therapeutic contacts.
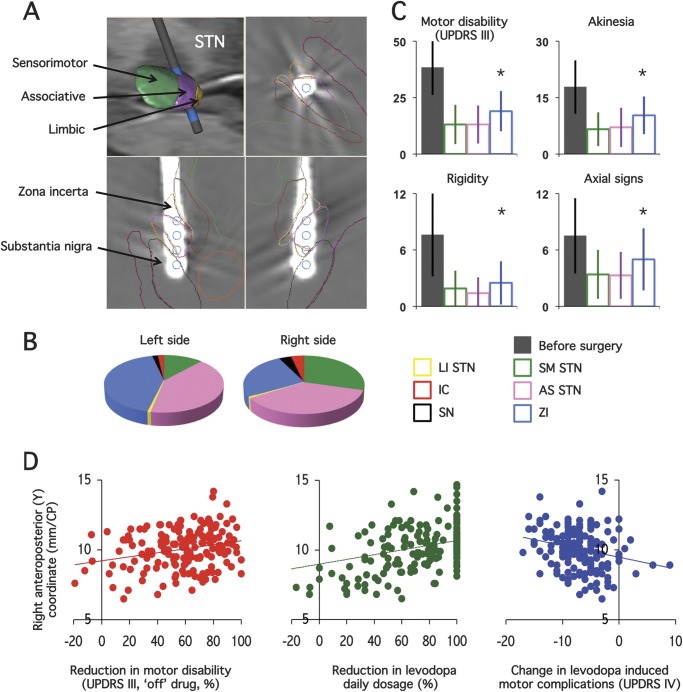
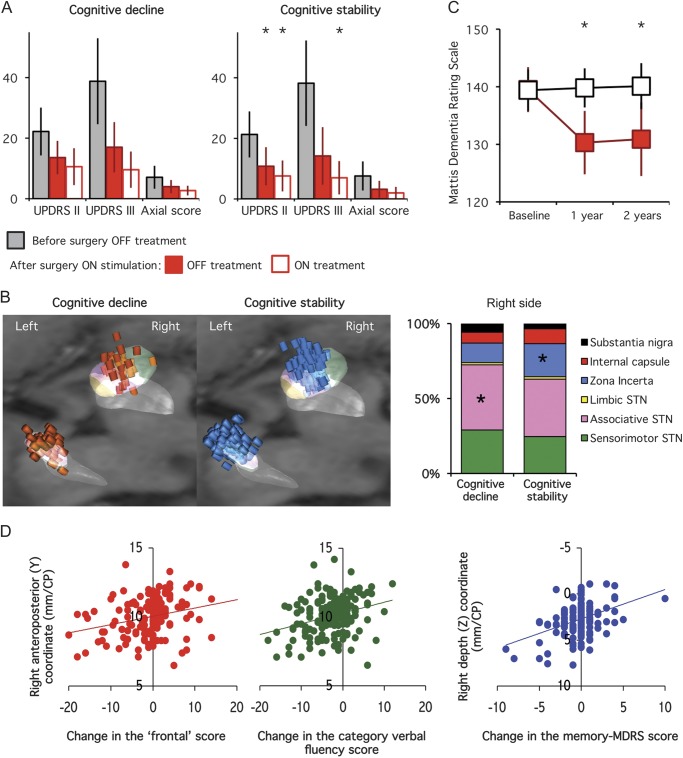
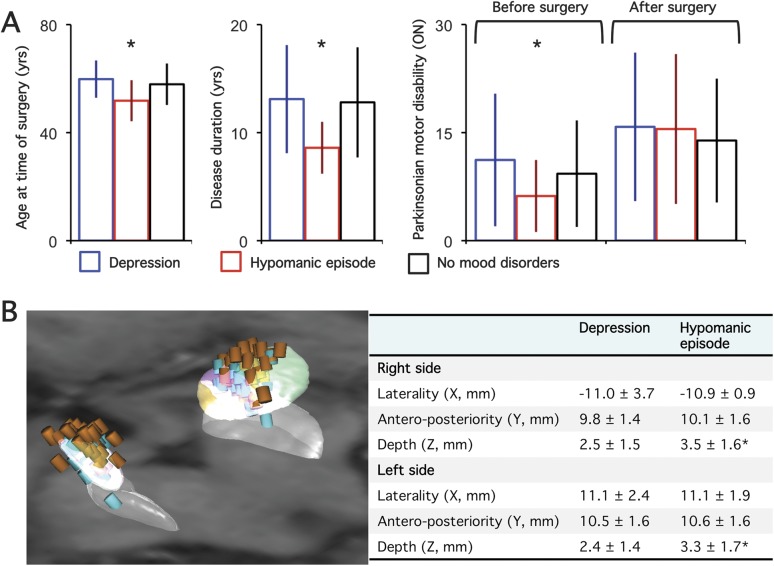
Results: Pre- and postoperative results were obtained in 262 patients with PD. The best motor outcome was obtained when stimulating contacts were located within the STN as compared with the zona incerta (64% vs 49% improvement). Eighteen percent of the patients presented a postoperative cognitive decline, which was found to be principally related to the surgical procedure. Other factors predictive of poor cognitive outcome were perioperative confusion and psychosis. Nineteen patients showed a stimulation-induced hypomania, which was related to both the form of the disease (younger age, shorter disease duration, higher levodopa responsiveness) and the ventral contact location. Postoperative depression was more frequent in patients already showing preoperative depressive and/or residual axial motor symptoms.
Conclusion: In this homogeneous cohort of patients with PD, we showed that (1) the STN is the best target to improve motor symptoms, (2) postoperative cognitive deficit is mainly related to the surgery itself, and (3) stimulation-induced hypomania is related to a combination of both the disease characteristics and a more ventral STN location.
Figures
References
-
- Limousin P, Krack P, Pollak P, et al. Electrical stimulation of the subthalamic nucleus in advanced Parkinson's disease. N Engl J Med 1998;339:1105–1111 - PubMed
-
- Parsons TD, Rogers SA, Braaten AJ, Woods SP, Troster AI. Cognitive sequelae of subthalamic nucleus deep brain stimulation in Parkinson's disease: a meta-analysis. Lancet Neurol 2006;5:578–588 - PubMed
-
- Voon V, Kubu C, Krack P, Houeto JL, Troster AI. Deep brain stimulation: neuropsychological and neuropsychiatric issues. Mov Disord 2006;21(suppl 14):S305–S327 - PubMed
-
- Daniels C, Krack P, Volkmann J, et al. Is improvement in the quality of life after subthalamic nucleus stimulation in Parkinson's disease predictable? Mov Disord 2011;26:2516–2521 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical