

Updated interim efficacy analysis and long-term safety of abiraterone acetate in metastatic castration-resistant prostate cancer patients without prior chemotherapy (COU-AA-302)
- PMID: 24647231
- PMCID: PMC4418928
- DOI: 10.1016/j.eururo.2014.02.056
Updated interim efficacy analysis and long-term safety of abiraterone acetate in metastatic castration-resistant prostate cancer patients without prior chemotherapy (COU-AA-302)
Abstract
Background: Abiraterone acetate (an androgen biosynthesis inhibitor) plus prednisone is approved for treating patients with metastatic castration-resistant prostate cancer (mCRPC). Study COU-AA-302 evaluated abiraterone acetate plus prednisone versus prednisone alone in mildly symptomatic or asymptomatic patients with progressive mCRPC without prior chemotherapy.
Objective: Report the prespecified third interim analysis (IA) of efficacy and safety outcomes in study COU-AA-302.
Design, setting, and participants: Study COU-AA-302, a double-blind placebo-controlled study, enrolled patients with mCRPC from April 2009 to June 2010. A total of 1088 patients were stratified by Eastern Cooperative Oncology Group performance status (0 vs 1).
Intervention: Patients were randomised 1:1 to abiraterone 1000mg plus prednisone 5mg twice daily by mouth versus prednisone.
Outcome measurements and statistical analysis: Co-primary end points were radiographic progression-free survival (rPFS) and overall survival (OS). Median times to event outcomes were estimated using the Kaplan-Meier method. Hazard ratios (HRs) and 95% confidence intervals (CIs) were derived using the Cox model, and treatment comparison used the log-rank test. The O'Brien-Fleming Lan-DeMets α-spending function was used for OS. Adverse events were summarised descriptively.
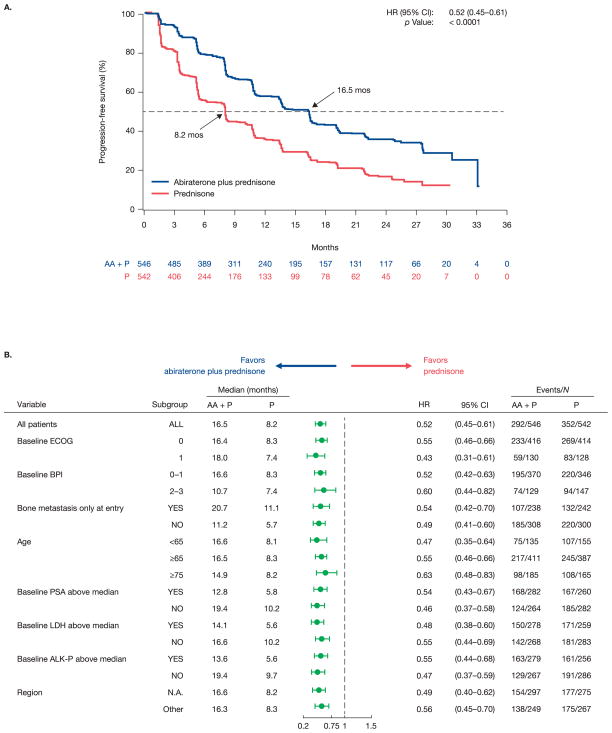
Results and limitations: With a median follow-up duration of 27.1 mo, improvement in rPFS was statistically significant with abiraterone treatment versus prednisone (median: 16.5 vs 8.2 mo; HR: 0.52 [95% CI, 0.45-0.61]; p<0.0001). Abiraterone improved OS (median: 35.3 vs 30.1 mo; HR: 0.79 [95% CI, 0.66-0.95]; p=0.0151) but did not reach the prespecified statistical efficacy boundary (α-level: 0.0035). A post hoc multivariate analysis for OS using known prognostic factors supported the primary results (HR: 0.74 [95% CI, 0.61-0.89]; p=0.0017), and all clinically relevant secondary end points and patient-reported outcomes improved. While the post hoc nature of the long-term safety analysis is a limitation, the safety profile with longer treatment exposure was consistent with prior reports.
Conclusions: The updated IA of study COU-AA-302 in patients with mCRPC without prior chemotherapy confirms that abiraterone delays disease progression, pain, and functional deterioration and has clinical benefit with a favourable safety profile, including in patients treated for ≥24 mo.
Trial registration: Study COU-AA-302, ClinicalTrials.gov number, NCT00887198.
Patient summary: The updated results of this ongoing study showed that disease progression was delayed in patients with advanced prostate cancer who were treated with abiraterone acetate and prednisone, and there was a continued trend in prolongation of life compared with patients treated with prednisone alone. Treatment with abiraterone acetate and prednisone was well tolerated by patients who were treated for >2 yr.
Keywords: Abiraterone acetate; Chemotherapy-naive; Efficacy; Metastatic castration-resistant prostate cancer; Safety.
Copyright © 2014 European Association of Urology. Published by Elsevier B.V. All rights reserved.
Figures



Comment in
-
Beyond approval: what is the most appropriate way to use the expanding Armamentarium in metastatic castration-resistant prostate cancer and how do we move forward?Eur Urol. 2014 Nov;66(5):826-8. doi: 10.1016/j.eururo.2014.03.046. Epub 2014 Apr 13. Eur Urol. 2014. PMID: 24751214 No abstract available.
References
-
- Heidenreich A, Bastian PJ, Bellmunt J, et al. EAU guidelines on prostate cancer, II: treatment of advanced, relapsing, and castration-resistant prostate cancer. Eur Urol. 2014;65:467–79. - PubMed
-
- National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology (NCCN guidelines) [Accessed May 28, 2013];Prostate cancer v. 2.2013. National Comprehensive Cancer Network Web site. http://www.nccn.org/professionals/physician_gls/pdf/prostate.pdf.
-
- Halabi S, Small EJ, Kantoff PW, et al. Prognostic model for predicting survival in men with hormone-refractory metastatic prostate cancer. J Clin Oncol. 2003;21:1232–7. - PubMed
-
- Tannock IF, de WR, Berry WR, et al. Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer. N Engl J Med. 2004;351:1502–12. - PubMed
-
- Petrylak DP, Tangen CM, Hussain MH, et al. Docetaxel and estramustine compared with mioxantrone and prednisone for advanced refractory prostate cancer. N Engl J Med. 2004;351:1513–20. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
