

Relative efficacy of mindfulness-based relapse prevention, standard relapse prevention, and treatment as usual for substance use disorders: a randomized clinical trial
- PMID: 24647726
- PMCID: PMC4489711
- DOI: 10.1001/jamapsychiatry.2013.4546
Relative efficacy of mindfulness-based relapse prevention, standard relapse prevention, and treatment as usual for substance use disorders: a randomized clinical trial
Abstract
Importance: Relapse is highly prevalent following substance abuse treatments, highlighting the need for improved aftercare interventions. Mindfulness-based relapse prevention (MBRP), a group-based psychosocial aftercare, integrates evidence-based practices from mindfulness-based interventions and cognitive-behavioral relapse prevention (RP) approaches.
Objective: To evaluate the long-term efficacy of MBRP in reducing relapse compared with RP and treatment as usual (TAU [12-step programming and psychoeducation]) during a 12-month follow-up period.
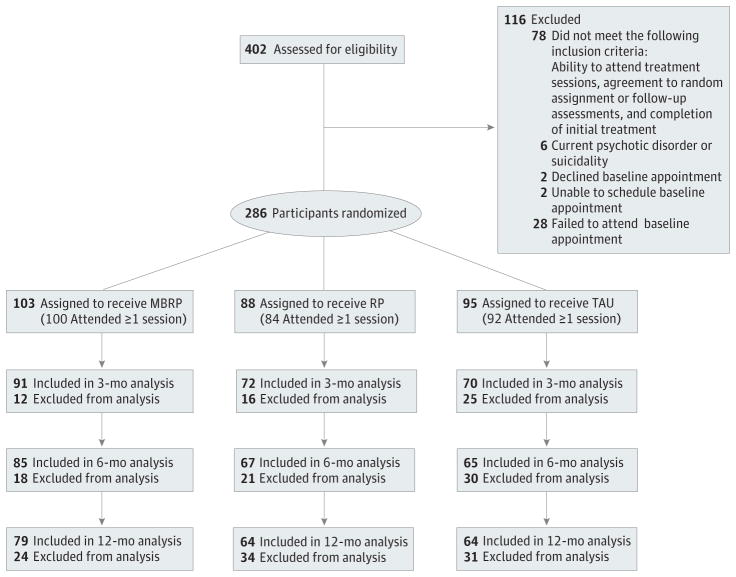
Design, setting, and participants: Between October 2009 and July 2012, a total of 286 eligible individuals who successfully completed initial treatment for substance use disorders at a private, nonprofit treatment facility were randomized to MBRP, RP, or TAU aftercare and monitored for 12 months. Participants medically cleared for continuing care were aged 18 to 70 years; 71.5% were male and 42.1% were of ethnic/racial minority.
Interventions: Participants were randomly assigned to 8 weekly group sessions of MBRP, cognitive-behavioral RP, or TAU.
Main outcomes and measures: Primary outcomes included relapse to drug use and heavy drinking as well as frequency of substance use in the past 90 days. Variables were assessed at baseline and at 3-, 6-, and 12-month follow-up points. Measures used included self-report of relapse and urinalysis drug and alcohol screenings.
Results: Compared with TAU, participants assigned to MBRP and RP reported significantly lower risk of relapse to substance use and heavy drinking and, among those who used substances, significantly fewer days of substance use and heavy drinking at the 6-month follow-up. Cognitive-behavioral RP showed an advantage over MBRP in time to first drug use. At the 12-month follow-up, MBRP participants reported significantly fewer days of substance use and significantly decreased heavy drinking compared with RP and TAU.
Conclusions and relevance: For individuals in aftercare following initial treatment for substance use disorders, RP and MBRP, compared with TAU, produced significantly reduced relapse risk to drug use and heavy drinking. Relapse prevention delayed time to first drug use at 6-month follow-up, with MBRP and RP participants who used alcohol also reporting significantly fewer heavy drinking days compared with TAU participants. At 12-month follow-up, MBRP offered added benefit over RP and TAU in reducing drug use and heavy drinking. Targeted mindfulness practices may support long-term outcomes by strengthening the ability to monitor and skillfully cope with discomfort associated with craving or negative affect, thus supporting long-term outcomes.
Trial registration: clinicaltrials.gov Identifier: NCT01159535
Conflict of interest statement
Figures
References
-
- Substance Abuse and Mental Health Services Administration. Treatment Episode Data Set (TEDS): 2005: Discharges From Substance Abuse Treatment Services: DASIS Series: S-41. Rockville, MD: Dept of Health & Human Services; 2008. Dept of Health & Human Services publication No. (SMA) 08-4314.
-
- McLellan AT, Lewis DC, O’Brien CP, Kleber HD. Drug dependence, a chronic medical illness: implications for treatment, insurance, and outcomes evaluation. JAMA. 2000;284(13):1689–1695. - PubMed
-
- Connors GJ, Maisto SA, Donovan DM. Conceptualizations of relapse: a summary of psychological and psychobiological models. Addiction. 1996;91(12 suppl):S5–S13. - PubMed
-
- Marlatt GA, Gordon JR. Relapse Prevention: Maintenance Strategies in the Treatment of Addictive Behaviors. New York, NY: Guilford Press; 1985.
-
- Brandon TH, Vidrine JI, Litvin EB. Relapse and relapse prevention. Annu Rev Clin Psychol. 2007;3:257–284. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- AA 019608-03/AA/NIAAA NIH HHS/United States
- F31 AA023126/AA/NIAAA NIH HHS/United States
- K01 AA021147/AA/NIAAA NIH HHS/United States
- UL1RR025014/RR/NCRR NIH HHS/United States
- UL1 RR025014/RR/NCRR NIH HHS/United States
- UL1 TR002319/TR/NCATS NIH HHS/United States
- R01 DA025764/DA/NIDA NIH HHS/United States
- K18 DA031464/DA/NIDA NIH HHS/United States
- 1K18DA031464-01/DA/NIDA NIH HHS/United States
- R21 DA019562/DA/NIDA NIH HHS/United States
- F31 AA019608/AA/NIAAA NIH HHS/United States
- 5R01DA025764-02/DA/NIDA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
