

Are articular cartilage lesions and meniscus tears predictive of IKDC, KOOS, and Marx activity level outcomes after anterior cruciate ligament reconstruction? A 6-year multicenter cohort study
- PMID: 24647881
- PMCID: PMC4195485
- DOI: 10.1177/0363546514525910
Are articular cartilage lesions and meniscus tears predictive of IKDC, KOOS, and Marx activity level outcomes after anterior cruciate ligament reconstruction? A 6-year multicenter cohort study
Abstract
Background: Identifying risk factors for inferior outcomes after anterior cruciate ligament reconstruction (ACLR) is important for prognosis and future treatment.
Hypothesis: Articular cartilage lesions and meniscus tears/treatment would predict International Knee Documentation Committee (IKDC) score, Knee injury and Osteoarthritis Outcome Score (KOOS) (all 5 subscales), and Marx activity level at 6 years after ACLR.
Study design: Cohort study (prognosis); Level of evidence, 1.
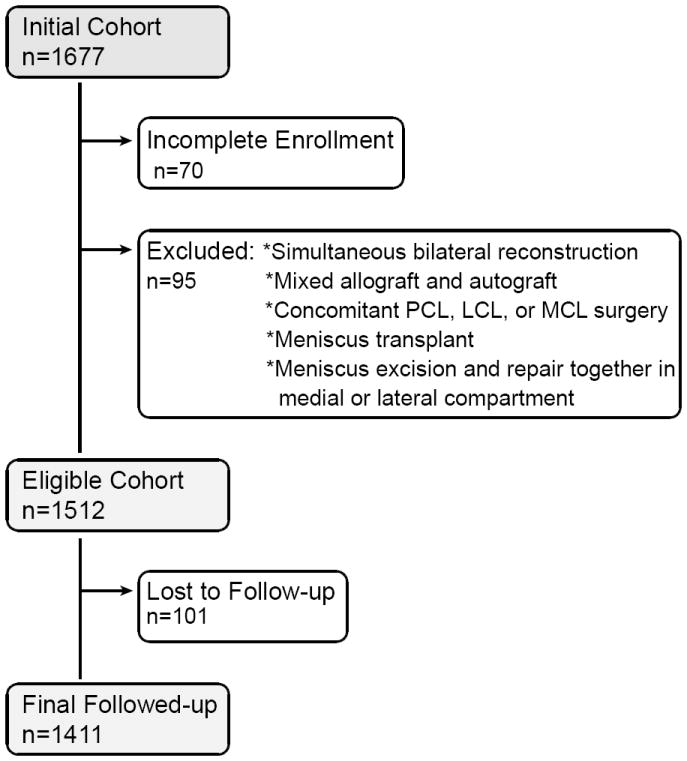
Methods: Between 2002 and 2004, a total of 1512 ACLR patients were prospectively enrolled and followed longitudinally, with the IKDC, KOOS, and Marx activity score completed at entry, 2 years, and 6 years. A logistic regression model was built incorporating variables from patient demographics, surgical technique, articular cartilage injuries, and meniscus tears/treatment to determine the predictors (risk factors) of IKDC and KOOS scores and Marx activity level at 6 years.
Results: A minimum follow-up on 86% (1307/1512) of the cohort was completed at 6 years. The cohort was 56% male and had a median age of 23 years at the time of enrollment, with 76% reporting a noncontact injury mechanism. Incidence of concomitant injury at the time of surgery consisted of the following: articular cartilage (medial femoral condyle [MFC], 25%; lateral femoral condyle [LFC] 20%; medial tibial plateau [MTP], 6%; lateral tibial plateau [LTP], 12%; patella, 20%; trochlear, 9%) and meniscus (medial, 38%; lateral, 46%). Both articular cartilage lesions and meniscus tears were significant predictors of 6-year outcomes on the IKDC and KOOS. Grade 3 or 4 articular cartilage lesions (excluding patella) significantly reduced IKDC and KOOS scores at 6 years. The IKDC demonstrated worse outcomes with the presence of a grade 3 or 4 chondral lesion on the MFC, MTP, and LFC. Likewise, the KOOS score was negatively affected by cartilage injury. The sole significant predictor of reduced Marx activity level was the presence of a grade 4 lesion on the MFC. Lateral meniscus repairs did not correlate with inferior results, but medial meniscus repairs predicted worse IKDC and KOOS scores. Lateral meniscus tears left alone significantly improved prognosis. Small partial meniscectomies (<33%) on the medial meniscus fared worse; conversely, larger excisions (>50%) on either the medial or lateral menisci improved prognosis. Analogous to previous studies, other significant predictors of lower outcome scores were lower baseline scores, higher body mass index, lower education level, smoking, and anterior cruciate ligament revisions.
Conclusion: Both articular cartilage injury and meniscus tears/treatment at the time of ACLR were significant predictors of IKDC and KOOS scores 6 years after ACLR. Similarly, having a grade 4 MFC lesion significantly reduced a patient's Marx activity level score at 6 years.
Keywords: ACL reconstruction; IKDC; KOOS; Marx activity rating scale; anterior cruciate ligament; articular cartilage, meniscus; outcomes.
Figures
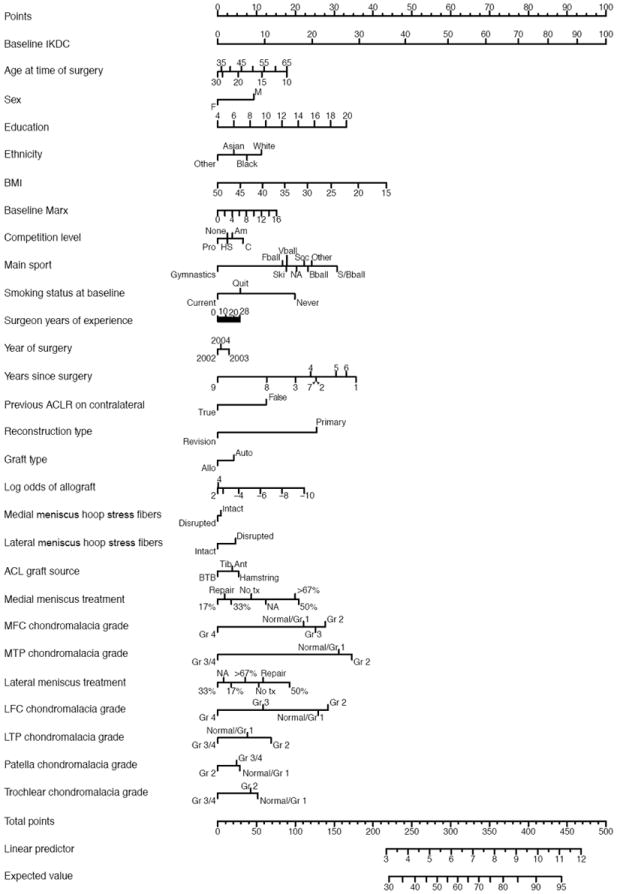
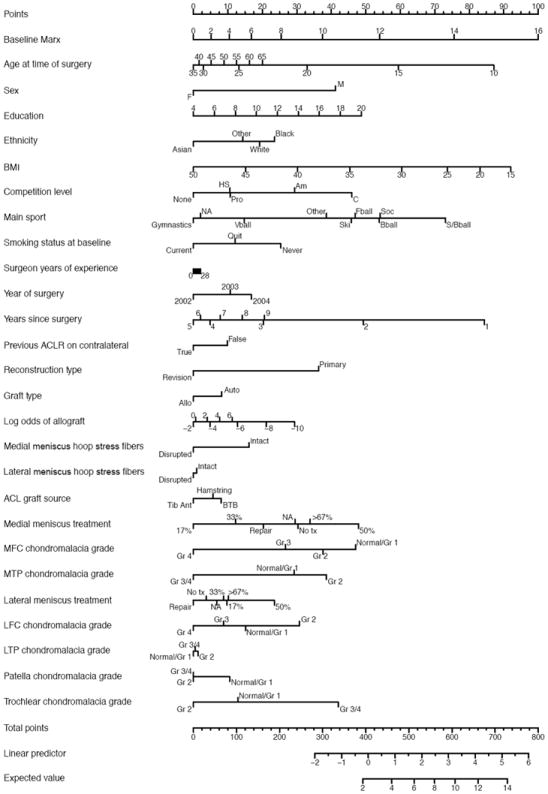
Baseline IKDC score (50) = 59 points
Age at the time of surgery (20 yrs) = 5 pts
Sex (male) = 9 pts
Education (16 years) = 25 pts
Ethnicity (white) = 11 pts
BMI (25) = 29 pts
Baseline Marx (12) = 11 pts
Competition level (high school) = 2.5 pts
Main sport (football) = 17 pts
Smoking status at baseline (current) = 0 pts
Surgeon years of experience (10 yrs) = 2 pts
Year of surgery (2004) = 1 pt
Years since surgery (3 yrs) = 20 pts
Previous ACLR on contralateral knee (false) = 12.5 pts
Reconstruction type (revision) = 0 pts
Graft type (autograft) = 4 pts
Log odds on allograft (2) = 0 pts
Medial meniscus hoop stress fibers (intact) = 1 pt
Lateral meniscus hoop stress fibers (intact) = 0 pts
ACL graft source (hamstring) = 5 pts
Medial meniscus treatment (repair) = 2 pts
MFC chondromalacia grade (grade 2) = 27.5 pts
MTP chondromalacia grade (normal/grade 1) = 31 pts
Lateral meniscus treatment (no treatment) = 10 pts
LFC chondromalacia grade (grade 4) = 0 pts
LTP chondromalacia grade (normal/grade 1) = 7.5 pts
Patella chondromalacia grade (grade 2) = 0 pts
Trochlear chondromalacia grade (grade 2) = 8 pts
References
-
- Barenius B, Forssblad M, Engstrom B, Eriksson K. Functional recovery after anterior cruciate ligament reconstruction, a study of health-related quality of life based on the Swedish National Knee Ligament Register. Knee Surg Sports Traumatol Arthrosc. 2013;21(4):914–27. - PubMed
-
- Borchers JR, Kaeding CC, Pedroza AD, Huston LJ, Spindler KP, Wright RW on behalf of the MOON Consortium and the MARS Group. Intra-articular findings in primary and revision anterior cruciate ligament reconstruction surgery: a comparison of the MOON and MARS study groups. Am J Sports Med. 2011;39(9):1889–93. - PMC - PubMed
-
- Claes S, Hermie L, Verdonk R, Bellemans J, Verdonk P. Is osteoarthritis an inevitable consequence of anterior cruciate ligament reconstruction? A meta-analysis. Knee Surg Sports Traumatol Arthrosc. 2012 Oct 26; Epub ahead of print. - PubMed
-
- Curl WW, Krome J, Gordon ES, Rushing J, Smith BP, Poehling GG. Cartilage injuries: a review of 31,516 knee arthroscopies. Arthroscopy. 1997;13(4):456–60. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
