

Acute respiratory failure in a 35-year-old woman following preterm vaginal delivery
- PMID: 24648478
- PMCID: PMC3962961
- DOI: 10.1136/bcr-2014-203676
Acute respiratory failure in a 35-year-old woman following preterm vaginal delivery
Abstract
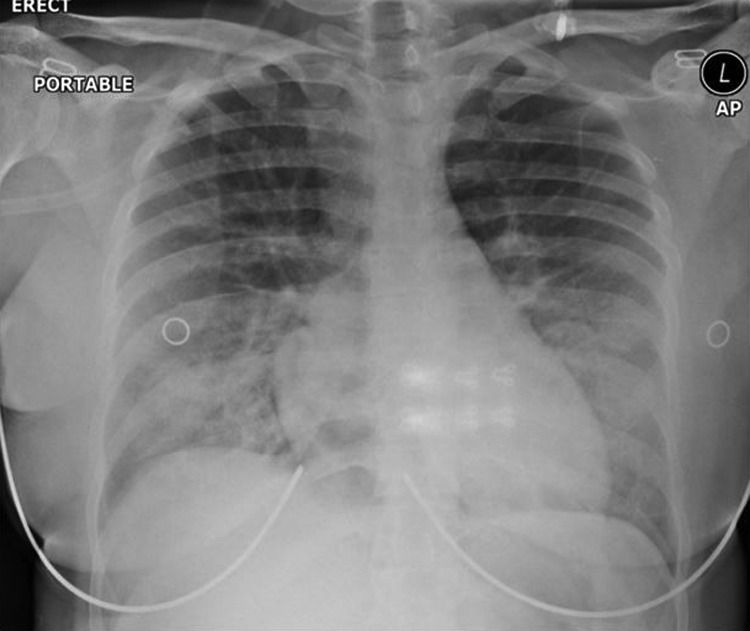
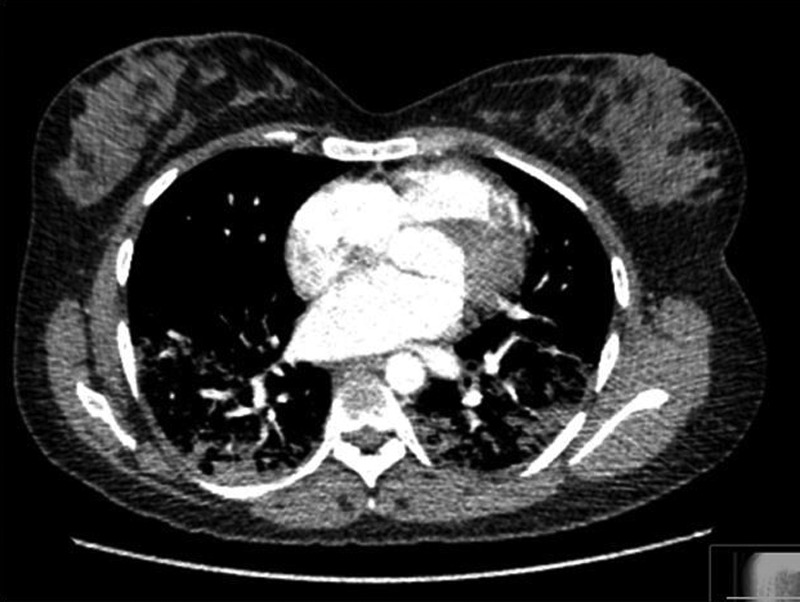
A 35-year-old woman, a non-smoker with a normal body mass index, 'felt wheezy' and developed profound hypoxia 30 min after preterm vaginal delivery at 24+ weeks of gestation. She denied other symptoms, had no fever but was tachycardic and tachypnoeic with normal blood pressure. Pulmonary embolism, amniotic fluid embolism, cardiomyopathy, arrhythmias, sepsis and non-cardiogenic pulmonary oedema were considered as differential diagnoses. Chest X-ray showed an increased pulmonary vasculature, but the blood tests, ECG, echocardiogram and CT pulmonary angiogram were essentially normal. She was managed on a high dependency area with high-flow oxygen and intravenous antibiotics. She improved dramatically and the oxygen requirements dropped to 2 L over the next 4 h. It is plausible that this woman had acute non-cardiogenic pulmonary oedema secondary to a combination of risk factors. This case highlights the importance of a methodical and multidisciplinary approach for a prompt diagnosis and successful treatment of an acutely ill parturient.
Figures

References
-
- Sciscione A, Ivester T, Largoza M, et al. Acute pulmonary edema in pregnancy. Obstet Gynecol 2003;101:511–15 - PubMed
-
- Poggi SH, Barr S, Cannum R, et al. Risk factors for pulmonary edema in triplet pregnancies. J Perinatol 2003;23:462–5 - PubMed
-
- Ogunyemi D. Risk factors for acute pulmonary edema in preterm delivery. Eur J Obstet Gynecol Reprod Biol 2007;133:143–7 - PubMed
-
- Cantwell R, Clutton-Brock T, Cooper G, et al. Saving mothers’ lives: reviewing maternal deaths to make motherhood safer: 2006–2008. The eighth report of the confidential enquiries into maternal deaths in the United Kingdom. BJOG 2011;118(Suppl 1):1–203 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical