

Concordance between molecular and phenotypic testing of Mycobacterium tuberculosis complex isolates for resistance to rifampin and isoniazid in the United States
- PMID: 24648563
- PMCID: PMC4042757
- DOI: 10.1128/JCM.00417-14
Concordance between molecular and phenotypic testing of Mycobacterium tuberculosis complex isolates for resistance to rifampin and isoniazid in the United States
Abstract
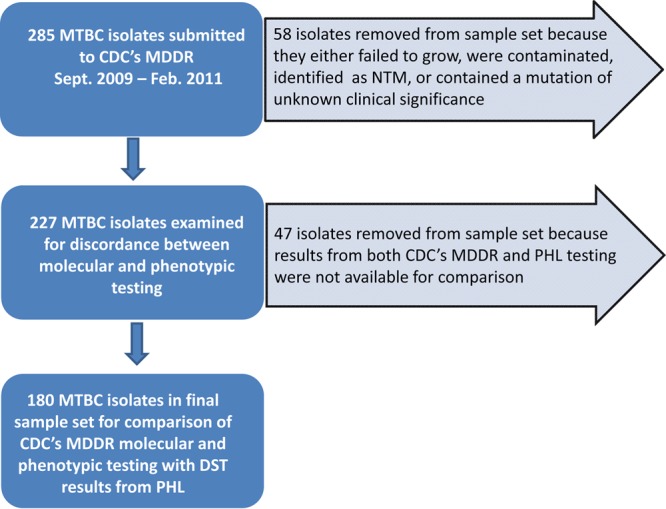
Multidrug-resistant (MDR) isolates of Mycobacterium tuberculosis complex (MTBC) are defined by resistance to at least rifampin (RMP) and isoniazid (INH). Rapid and accurate detection of multidrug resistance is essential for effective treatment and interruption of disease transmission of tuberculosis (TB). Overdiagnosis of MDR TB may result in treatment with second-line drugs that are more costly, less effective, and more poorly tolerated than first-line drugs. CDC offers rapid confirmation of MDR TB by the molecular detection of drug resistance (MDDR) for mutations associated with resistance to RMP and INH along with analysis for resistance to other first-line and second-line drugs. Simultaneously, CDC does growth-based phenotypic drug susceptibility testing (DST) by the indirect agar proportion method for a panel of first-line and second-line antituberculosis drugs. We reviewed discordance between molecular and phenotypic DST for INH and RMP for 285 isolates submitted as MTBC to CDC from September 2009 to February 2011. We compared CDC's results with those from the submitting public health laboratories (PHL). Concordances between molecular and phenotypic testing at CDC were 97.4% for RMP and 92.5% for INH resistance. Concordances between CDC's molecular testing and PHL DST results were 93.9% for RMP and 90.0% for INH. Overall concordance between CDC molecular and PHL DST results was 91.7% for RMP and INH collectively. Discordance was primarily attributable to the absence of known INH resistance mutations in isolates found to be INH resistant by DST and detection of mutations associated with low-level RMP resistance in isolates that were RMP susceptible by phenotypic DST. Both molecular and phenotypic test results should be considered for the diagnosis of MDR TB.
Copyright © 2014, American Society for Microbiology. All Rights Reserved.
Figures
References
-
- Blumberg HM, Burman WJ, Chaisson RE, Daley CL, Etkind SC, Friedman LN, Fujiwara P, Grzemska M, Hopewell PC, Iseman MD, Jasmer RM, Koppaka V, Menzies RI, O'Brien RJ, Reves RR, Reichman LB, Simone PM, Starke JR, Vernon AA; American Thoracic Society, Centers for Disease Control and Prevention and the Infectious Diseases Society. 2003. American Thoracic Society/ Centers for Disease Control and Prevention/Infectious Diseases Society of America: treatment of tuberculosis. Am. J. Crit. Respir. Care Med. 167:603–662. 10.1164/rccm.167.4.603 - DOI - PubMed
-
- Campbell PJ, Morlock GP, Sikes DR, Dalton TL, Metchock B, Starks AM, Hooks DP, Cowan LS, Plikaytis BB, Posey JE. 2011. Molecular detection of mutations associated with first- and second-line drug resistance compared with conventional drug susceptibility testing of Mycobacterium tuberculosis. Antimicrob. Agents Chemother. 55:2032–2041. 10.1128/AAC.01550-10 - DOI - PMC - PubMed
-
- Driscoll J, Lentz A, Sikes D, Metchock B. 2010. The first month of a new diagnostic service for the molecular detection of MDR and XDR tuberculosis. Am. J. Respir. Crit. Care Med. 181:A2259 http://www.atsjournals.org/doi/abs/10.1164/ajrccm-conference.2010.181.1_... - DOI
-
- Clinical and Laboratory Standards Institute. 2011. Susceptibility testing of Mycobacteria, Nocardia, and other aerobic Actinomycetes; approved standard—2nd ed, p 1–64 CLSI document M24A2E, vol 31, no 5 Clinical and Laboratory Standards Institute, Wayne, PA - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
