

A comparison of 1 minimum alveolar concentration desflurane and 1 minimum alveolar concentration isoflurane anesthesia in patients undergoing craniotomy for supratentorial lesions
- PMID: 24648575
- PMCID: PMC3955242
- DOI: 10.1016/j.curtheres.2011.03.001
A comparison of 1 minimum alveolar concentration desflurane and 1 minimum alveolar concentration isoflurane anesthesia in patients undergoing craniotomy for supratentorial lesions
Abstract
Background: A critical point in craniotomy is during opening of the dura and the subsequent potential for cerebral edema. Use of desflurane in neurosurgery may be beneficial because it facilitates early postoperative neurologic evaluation; however, data on the effect of desflurane on intracranial pressure in humans are limited. Isoflurane has been used extensively in neurosurgical patients.
Objective: This study compared 1 minimum alveolar concentration (MAC) desflurane with 1 MAC isoflurane in facilitating hemodynamic stability, brain relaxation, and postoperative recovery characteristics in patients who underwent craniotomy for supratentorial lesions.
Methods: A total of 70 patients (aged 18-65 years), with American Society of Anesthesiologists (ASA) 1 or 2 physical status, who underwent craniotomy for supratentorial lesions, were enrolled in the study. For induction of anesthesia, fentanyl (2 μg/kg IV) and propofol (2 mg/kg IV) were administered. Endotracheal intubation was performed after administration of vecuronium (0.1 mg/kg IV) for total muscle relaxation. Before insertion of the skull pins, additional fentanyl (2 μg/kg IV) was administered. Patients were randomly allocated to 1 of 2 anesthetic regimens. For maintenance of anesthesia, 35 patients received 1 MAC of desflurane (group 1) and 35 patients received 1 MAC of isoflurane (group 2) within 50% oxygen in nitrous oxide. Intraoperatively, heart rate (HR) and mean arterial pressure (MAP) were measured and recorded before induction and 1 minute after induction, after endotracheal intubation, before skull pin insertion and 1 minute after skull pin insertion, before incision and 1 minute after incision, and before extubation and 1 minute after extubation. Also, HR and MAP were recorded at 30-minute intervals. Postoperatively, extubation time, eye opening time to verbal stimuli, orientation time, and time to reach an Aldrete postanesthetic recovery score of ≥8 were recorded. In addition, opioid consumption was calculated and recorded. Brain relaxation was evaluated according to a 4-step brain relaxation scoring scale. All outcomes of the study were assessed and recorded by an anesthesiologist blinded to the volatile anesthetic gases studied.
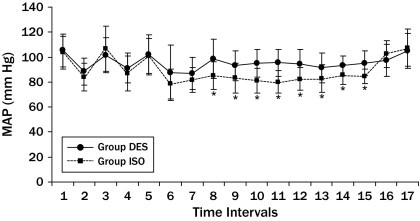
Results: No significant difference in HR was observed between the 2 groups. Intraoperative MAP values in group 1 were higher than in group 2 (P < 0.05). No significant difference was found between these groups in brain relaxation and opioid consumption. Extubation time, eye opening time to verbal stimuli, and time to reach an Aldrete score of ≥8 were found to be significantly shorter in patients in group 1 compared with patients in group 2 (P < 0.05).
Conclusions: In patients who underwent craniotomy for supratentorial lesions, patients who received 1 MAC desflurane-based anesthesia had earlier postoperative cognitive recovery and postoperative neurologic examination compared with patients who received 1 MAC isoflurane-based anesthesia. The observed benefits of early recovery from anesthesia, however, should be considered with risks such as higher MAP in patients administered 1 MAC desflurane.
Keywords: desflurane; hemodynamic stability; isoflurane; neuroanesthesia; postoperative recovery.
Figures

Similar articles
-
A comparison between sevoflurane and desflurane anesthesia in patients undergoing craniotomy for supratentorial intracranial surgery.Anesth Analg. 2009 Aug;109(2):567-71. doi: 10.1213/ane.0b013e3181ac1265. Anesth Analg. 2009. PMID: 19608833 Clinical Trial.
-
Awakening properties of isoflurane, sevoflurane, and desflurane in pediatric patients after craniotomy for supratentorial tumours.J Neurosurg Anesthesiol. 2015 Jan;27(1):1-6. doi: 10.1097/ANA.0000000000000058. J Neurosurg Anesthesiol. 2015. PMID: 24633212 Clinical Trial.
-
[Effects of desflurane and sevoflurane anesthesia on postoperative recovery after long-term tumor surgery].Zhonghua Yi Xue Za Zhi. 2020 Aug 4;100(29):2278-2282. doi: 10.3760/cma.j.cn112137-20200422-01273. Zhonghua Yi Xue Za Zhi. 2020. PMID: 32746598 Clinical Trial. Chinese.
-
Clinical Effects and Adverse Events Associated With Desflurane Use in Adult Patients Undergoing Supratentorial Craniotomy: A Systematic Review.J Neurosurg Anesthesiol. 2024 Jan 1;36(1):20-28. doi: 10.1097/ANA.0000000000000905. Epub 2023 Jan 30. J Neurosurg Anesthesiol. 2024. PMID: 36706431
-
Anesthetic Management of Asleep and Awake Craniotomy for Supratentorial Tumor Resection.Anesthesiol Clin. 2021 Mar;39(1):71-92. doi: 10.1016/j.anclin.2020.11.007. Anesthesiol Clin. 2021. PMID: 33563387 Review.
Cited by
-
Neurosurgical Anesthesia: Optimizing Outcomes with Agent Selection.Biomedicines. 2023 Jan 27;11(2):372. doi: 10.3390/biomedicines11020372. Biomedicines. 2023. PMID: 36830909 Free PMC article. Review.
-
Effects of avoiding neuromuscular blocking agents during maintenance of anaesthesia on recovery characteristics in patients undergoing craniotomy for supratentorial lesions: A randomised controlled study.Indian J Anaesth. 2017 Jan;61(1):42-47. doi: 10.4103/0019-5049.198408. Indian J Anaesth. 2017. PMID: 28216703 Free PMC article.
-
Comparison of propofol and inhalational anaesthetics for brain relaxation in neurosurgery: A systematic review and network meta-analysis.Indian J Anaesth. 2025 Aug;69(8):770-778. doi: 10.4103/ija.ija_189_25. Epub 2025 Jul 10. Indian J Anaesth. 2025. PMID: 40800708 Free PMC article.
-
Comparison of intravenous labetalol and bupivacaine scalp block on the hemodynamic and entropy changes following skull pin application: A randomized, open label clinical trial.Asian J Neurosurg. 2016 Jan-Mar;11(1):60-5. doi: 10.4103/1793-5482.165801. Asian J Neurosurg. 2016. PMID: 26889282 Free PMC article.
References
-
- Petersen K.D., Landsfeld U., Cold G.E. Intracranial pressure and cerebral hemodynamic in patients with cerebral tumors: a randomized prospective study of patients subjected to craniotomy in propofol-fentanyl, isoflurane-fentanyl, or sevoflurane-fentanyl anesthesia. Anesthesiology. 2003;98:329–336. - PubMed
-
- Coles J.P., Leary T.S., Monteiro J.N. Propofol anesthesia for craniotomy: a double blind comparison of remifentanil, alfentanil, and fentanyl. J Neurosurg Anesthesiol. 2000;12:15–20. - PubMed
-
- Bruder N., Ravussin P. Recovery from anesthesia and postoperative extubation of neurosurgical patients: A review. J Neurosurg Anesthesiol. 1999;11:282–293. - PubMed
-
- Talke P., Caldwell J., Dodsont B., Richardson A. Desflurane and isoflurane increase lumbar cerebrospinal fluid pressure in normocapnic patients undergoing transsphenoidal hypophysectomy. Anesthesiology. 1996;85:999–1004. - PubMed
-
- Ornstein E., Young W.L., Fleicher L.H., Ostapkovich N. Desflurane and isoflurane have similar effects on cerebral blood flow in patients with intracranial mass lesions. Anesthesiology. 1993;79:498–502. - PubMed
LinkOut - more resources
Full Text Sources
