

Propofol infusion syndrome in refractory status epilepticus
- PMID: 24649467
- PMCID: PMC3957310
- DOI: 10.14581/jer.13004
Propofol infusion syndrome in refractory status epilepticus
Abstract
Background and purpose: Propofol is used for treating refractory status epilepticus, which has high rate of mortality. Propofol infusion syndrome is a rare but often fatal syndrome, characterized by lactic acidosis, lipidemia, and cardiac failure, associated with propofol infusion over prolonged periods of time. We investigated the clinical factors that characterize propofol infusion syndrome to know the risk of them in refractory status epilepticus.
Methods: This retrospective observation study was conducted in Samsung medical center from Jan. 2005 to Dec. 2009. Thirty two patients (19 males, 13 females, aged between 16 and 64 years), with refractory status epilepsy were included. Their clinical findings and treatment outcomes were evaluated retrospectively. We divided our patients into established status epilepticus (ESE) and refractory status epilepticus (RSE). And then the patients with RSE was further subdivided into propofol treatment group (RSE-P) and the other anesthetics treatment group (RSE-O). We analyzed the clinical characteristics by comparison of the groups.
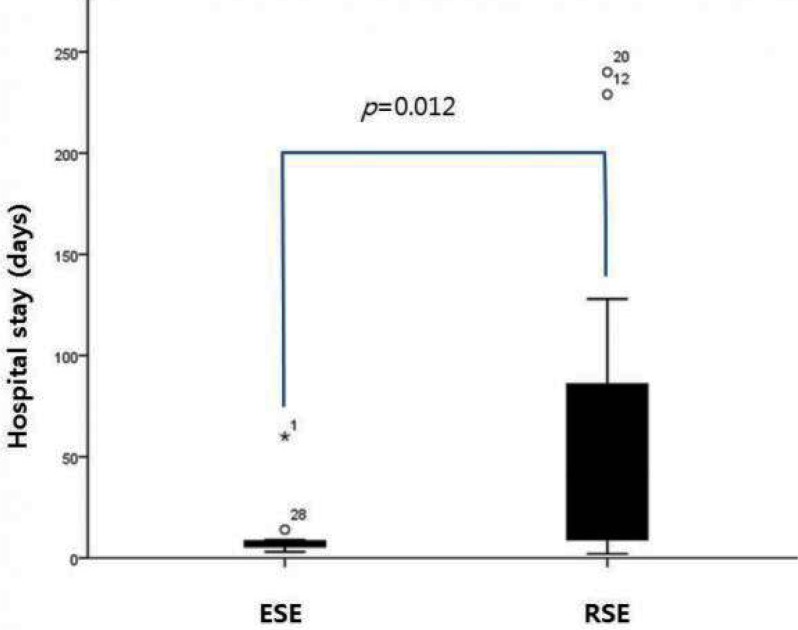
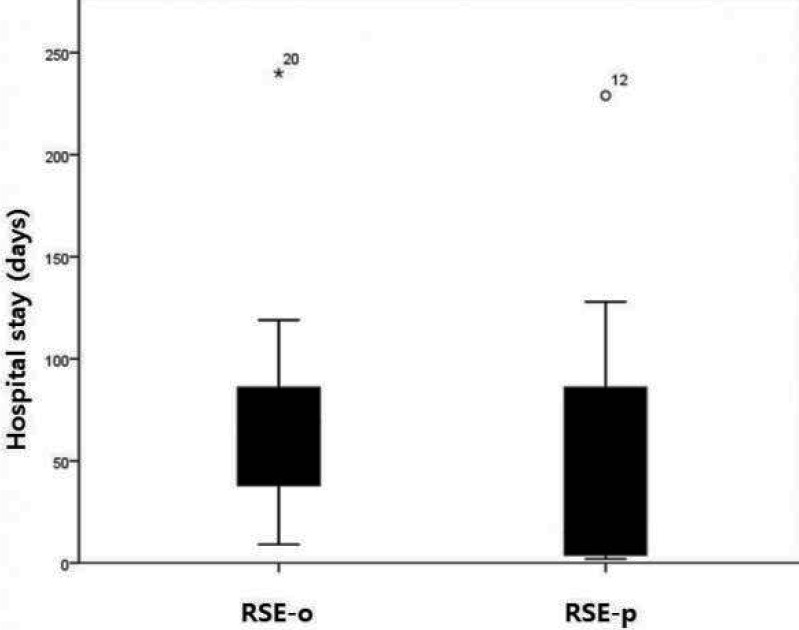
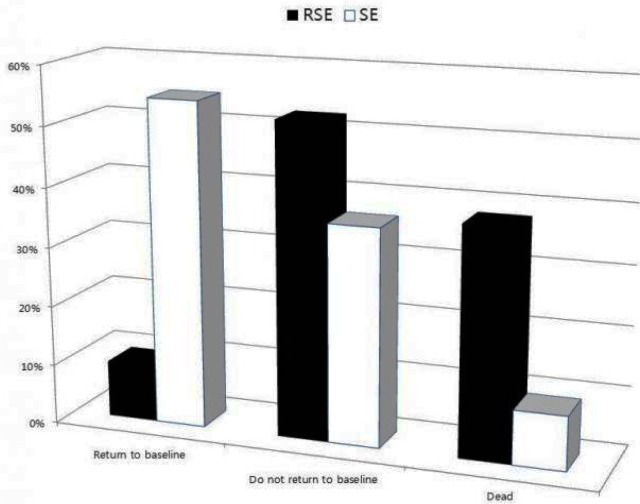
Results: There were significant differences of hypotension and lipid change between ESE and RSE (p<0.05). However, there was no significant difference between RSE-P and RSE-O groups. The hospital days were longer in RSE than in ESE (p=0.012) and treatment outcome was also worse in RSE than in ESE (p=0.007) but there were no significant differences of hospital stays and treatment outcome between RSE-P and RSE-O.
Conclusions: RSE is very critical disease with high mortality, which may show as many clinical changes as propofol infusion syndrome. Therefore propofol infusion syndrome might be considered as one of the clinical manifestations of RSE.
Keywords: Anesthetics; Propofol infusion syndrome; Status Epilepticus.
Figures


References
-
- Bleck TP. Management approaches to prolonged seizures and status epilepticus. Epilepsia. 1999;40(Suppl 1):S59–63. - PubMed
-
- Brown LA, Levin GM. Role of propofol in refractory status epilepticus. Ann Pharmacother. 1998;32:1053–59. - PubMed
-
- Mayer SA, Claassen J, Lokin J, Mendelsohn F, Dennis LJ, Fitzsimmons BF. Refractory status epilepticus: frequency, risk factors, and impact on outcome. Archives of Neurology. 2002;59:205–10. - PubMed
-
- Chen JW, Wasterlain CG. Status epilepticus: pathophysiology and management in adults. Lancet Neurology. 2006;5:246–56. - PubMed
-
- Niermeijer JM, Uiterwaal CS, Van Donselaar CA. Propofol in status epilepticus: little evidence, many dangers? Journal of Neurology. 2003;250:1237–40. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
