

Lassa fever in post-conflict sierra leone
- PMID: 24651047
- PMCID: PMC3961205
- DOI: 10.1371/journal.pntd.0002748
Lassa fever in post-conflict sierra leone
Abstract
Background: Lassa fever (LF), an often-fatal hemorrhagic disease caused by Lassa virus (LASV), is a major public health threat in West Africa. When the violent civil conflict in Sierra Leone (1991 to 2002) ended, an international consortium assisted in restoration of the LF program at Kenema Government Hospital (KGH) in an area with the world's highest incidence of the disease.
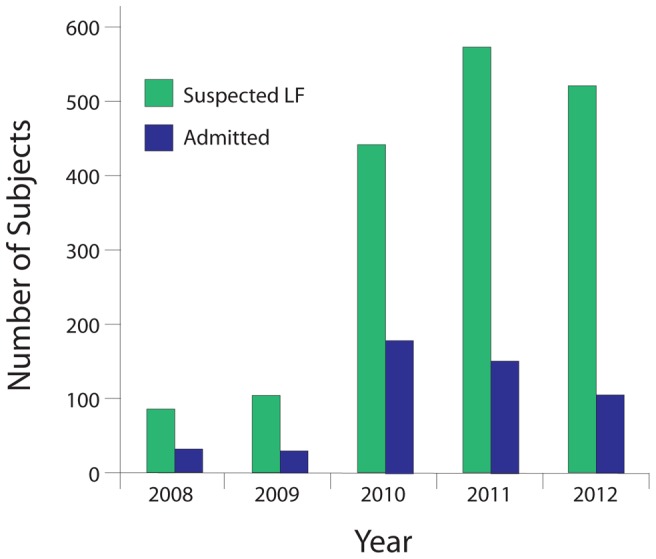
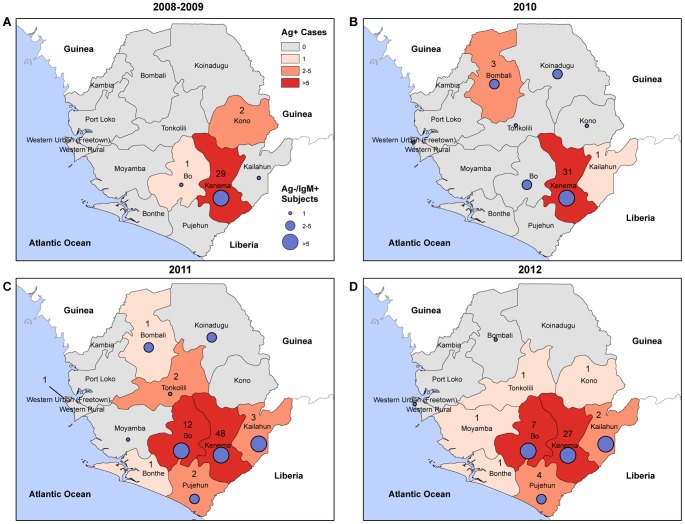
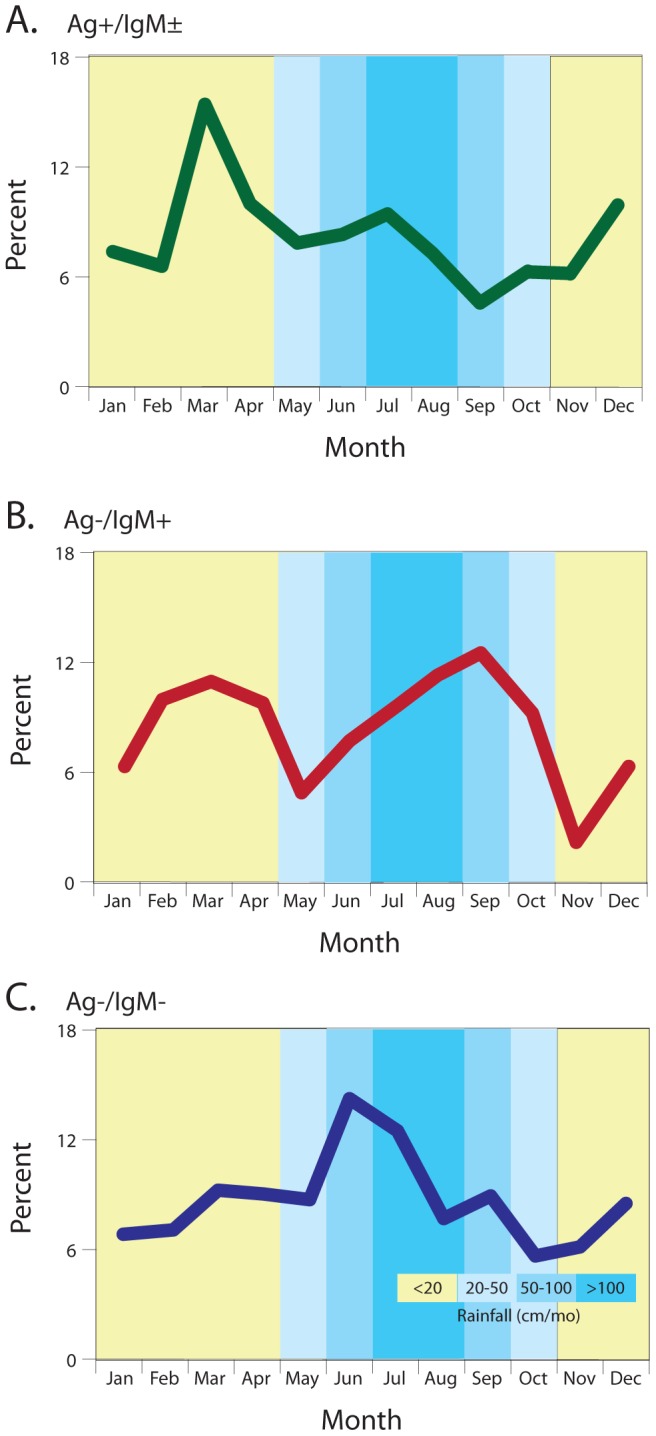
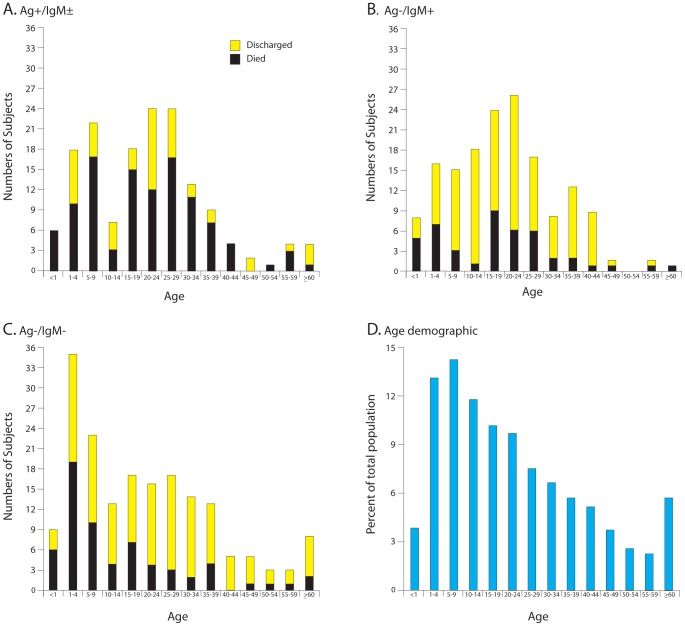
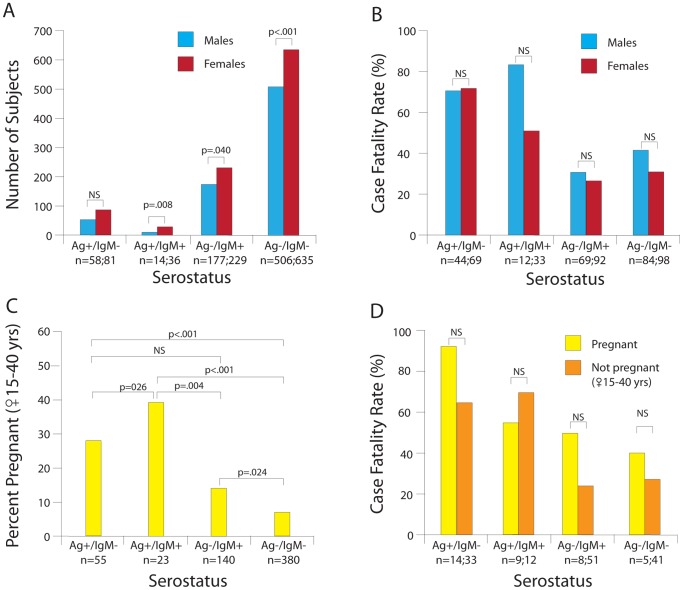
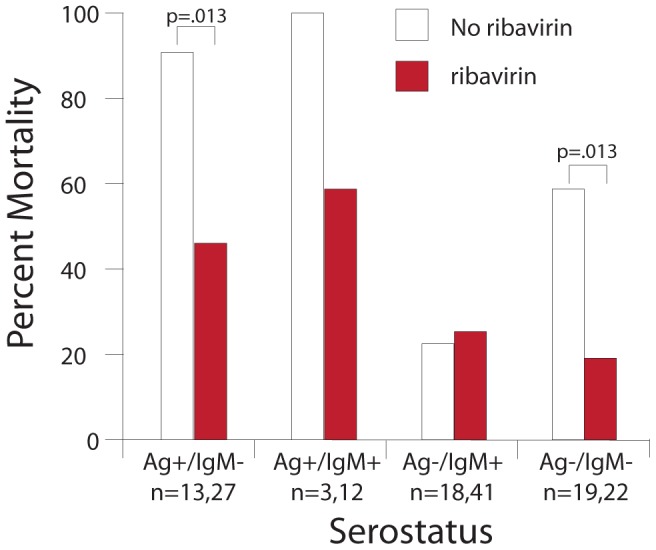
Methodology/principal findings: Clinical and laboratory records of patients presenting to the KGH Lassa Ward in the post-conflict period were organized electronically. Recombinant antigen-based LF immunoassays were used to assess LASV antigenemia and LASV-specific antibodies in patients who met criteria for suspected LF. KGH has been reestablished as a center for LF treatment and research, with over 500 suspected cases now presenting yearly. Higher case fatality rates (CFRs) in LF patients were observed compared to studies conducted prior to the civil conflict. Different criteria for defining LF stages and differences in sensitivity of assays likely account for these differences. The highest incidence of LF in Sierra Leone was observed during the dry season. LF cases were observed in ten of Sierra Leone's thirteen districts, with numerous cases from outside the traditional endemic zone. Deaths in patients presenting with LASV antigenemia were skewed towards individuals less than 29 years of age. Women self-reporting as pregnant were significantly overrepresented among LASV antigenemic patients. The CFR of ribavirin-treated patients presenting early in acute infection was lower than in untreated subjects.
Conclusions/significance: Lassa fever remains a major public health threat in Sierra Leone. Outreach activities should expand because LF may be more widespread in Sierra Leone than previously recognized. Enhanced case finding to ensure rapid diagnosis and treatment is imperative to reduce mortality. Even with ribavirin treatment, there was a high rate of fatalities underscoring the need to develop more effective and/or supplemental treatments for LF.
Conflict of interest statement
We have read the journal's policy and have the following conflicts. The Viral Hemorrhagic Fever Consortium (vhfc.org) is a partnership of academic and industry scientists who are developing diagnostics, therapeutics and vaccines for LF and other severe diseases. Tulane University and various industry partners have filed United States and foreign patent applications on behalf of the consortium for several of these technologies. If commercial products are developed, consortium members may receive royalties or profits. This does not alter our adherence to all PLOS policies on sharing data and materials.
Figures
Comment in
-
After the “blood diamond” conflict: lassa fever in Sierra Leone.Clin Infect Dis. 2014 Dec 15;59(12):iii-iv. Clin Infect Dis. 2014. PMID: 25574547 No abstract available.
References
-
- Buckley SM, Casals J (1970) Lassa fever, a new virus disease of man from West Africa. 3. Isolation and characterization of the virus. Am J Trop Med Hyg 19: 680–691. - PubMed
-
- Watts GM (2013) Lily Lyman Pinneo. The Lancet 380: 1552.
-
- Bausch DG, Demby AH, Coulibaly M, Kanu J, Goba A, et al. (2001) Lassa fever in Guinea: I. Epidemiology of human disease and clinical observations. Vector Borne Zoonotic Dis 1: 269–281. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- AI2009061/AI/NIAID NIH HHS/United States
- AI082119/AI/NIAID NIH HHS/United States
- R13 AI104216/AI/NIAID NIH HHS/United States
- AI067188/AI/NIAID NIH HHS/United States
- U19 AI109762/AI/NIAID NIH HHS/United States
- HHSN272200900049C/AI/NIAID NIH HHS/United States
- P20 GM103501/GM/NIGMS NIH HHS/United States
- U19 AI115589/AI/NIAID NIH HHS/United States
- P20GM103501/GM/NIGMS NIH HHS/United States
- U01 AI082119/AI/NIAID NIH HHS/United States
- HHSN272200900018C/AI/NIAID NIH HHS/United States
- AI104621/AI/NIAID NIH HHS/United States
- UC7 AI094660/AI/NIAID NIH HHS/United States
- AI104216/AI/NIAID NIH HHS/United States
- AI2008031/AI/NIAID NIH HHS/United States
- HHSN272201000022C/AI/NIAID NIH HHS/United States
- R01 AI104621/AI/NIAID NIH HHS/United States
- UC1 AI067188/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
