

A mixed methods study of a health worker training intervention to increase syndromic referral for gambiense human African trypanosomiasis in South Sudan
- PMID: 24651696
- PMCID: PMC3961197
- DOI: 10.1371/journal.pntd.0002742
A mixed methods study of a health worker training intervention to increase syndromic referral for gambiense human African trypanosomiasis in South Sudan
Abstract
Background: Active screening by mobile teams is considered the most effective method for detecting gambiense-type human African trypanosomiasis (HAT) but constrained funding in many post-conflict countries limits this approach. Non-specialist health care workers (HCWs) in peripheral health facilities could be trained to identify potential cases for testing based on symptoms. We tested a training intervention for HCWs in peripheral facilities in Nimule, South Sudan to increase knowledge of HAT symptomatology and the rate of syndromic referrals to a central screening and treatment centre.
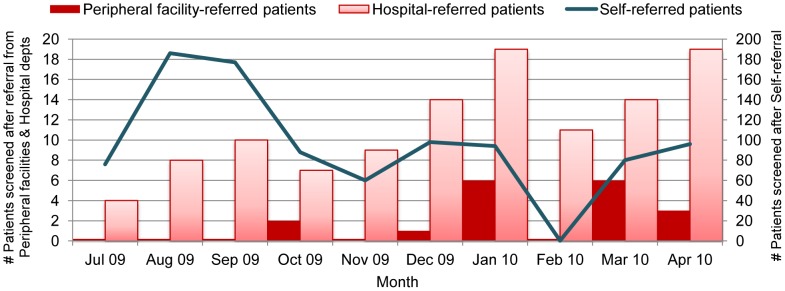
Methodology/principal findings: We trained 108 HCWs from 61/74 of the public, private and military peripheral health facilities in the county during six one-day workshops and assessed behaviour change using quantitative and qualitative methods. In four months prior to training, only 2/562 people passively screened for HAT were referred from a peripheral HCW (0 cases detected) compared to 13/352 (2 cases detected) in the four months after, a 6.5-fold increase in the referral rate observed by the hospital. Modest increases in absolute referrals received, however, concealed higher levels of referral activity in the periphery. HCWs in 71.4% of facilities followed-up had made referrals, incorporating new and pre-existing ideas about HAT case detection into referral practice. HCW knowledge scores of HAT symptoms improved across all demographic sub-groups. Of 71 HAT referrals made, two-thirds were from new referrers. Only 11 patients completed the referral, largely because of difficulties patients in remote areas faced accessing transportation.
Conclusions/significance: The training increased knowledge and this led to more widespread appropriate HAT referrals from a low base. Many referrals were not completed, however. Increasing access to screening and/or diagnostic tests in the periphery will be needed for greater impact on case-detection in this context. These data suggest it may be possible for peripheral HCWs to target the use of rapid diagnostic tests for HAT.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures



References
-
- Blum J, Schmid C, Burri C (2006) Clinical aspects of 2541 patients with second stage human African trypanosomiasis. Acta Trop 97: 55–64. - PubMed
-
- Dumas M, Bisser S (1999) Chapter 13: Clinical aspects of human African trypanosomiasis. In: Dumas M, Bonteille B, Buguet A, editors. Progress in human African trypanosomiasis, sleeping sickness. Paris: Springer-Verlag France.
-
- Jannin JG, Simarro PP, Franco JR (2011) A11 Progress in control and elimination of human African trypanosomiasis, 2010. In: Choffnes E, Relman D, editors. National Academies Press.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
