

Association of body mass index with outcomes in patients with CKD
- PMID: 24652789
- PMCID: PMC4147974
- DOI: 10.1681/ASN.2013070754
Association of body mass index with outcomes in patients with CKD
Abstract
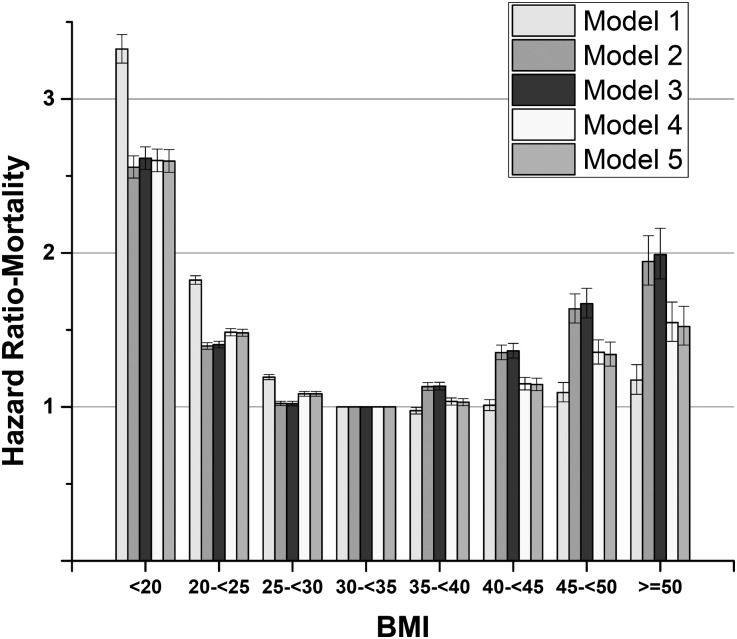
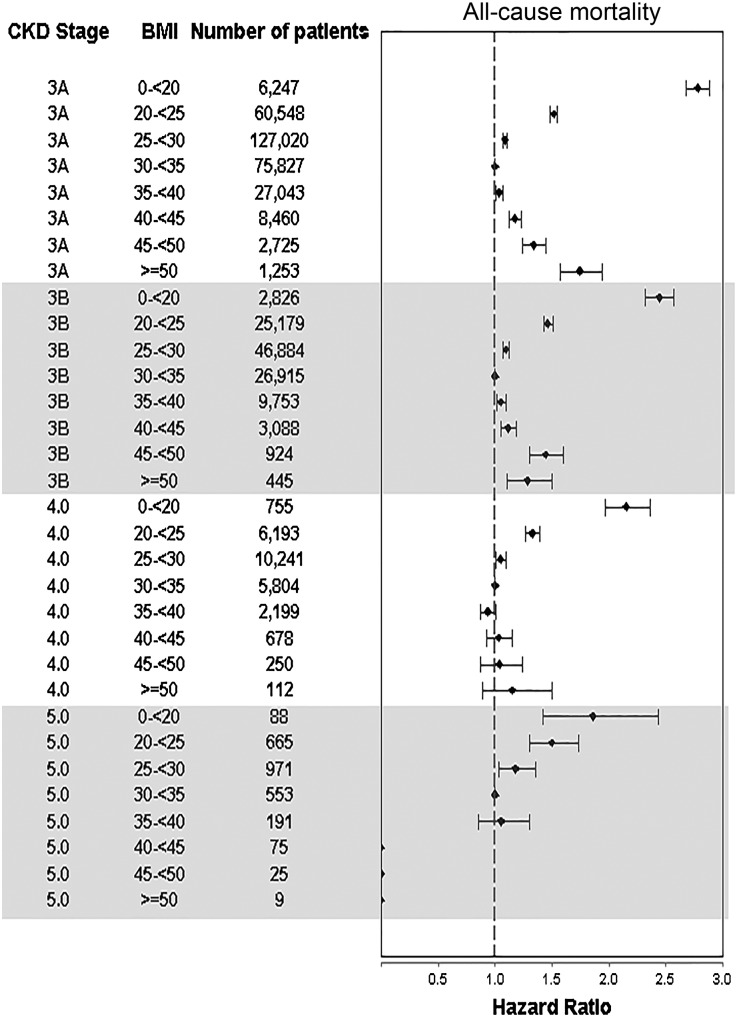
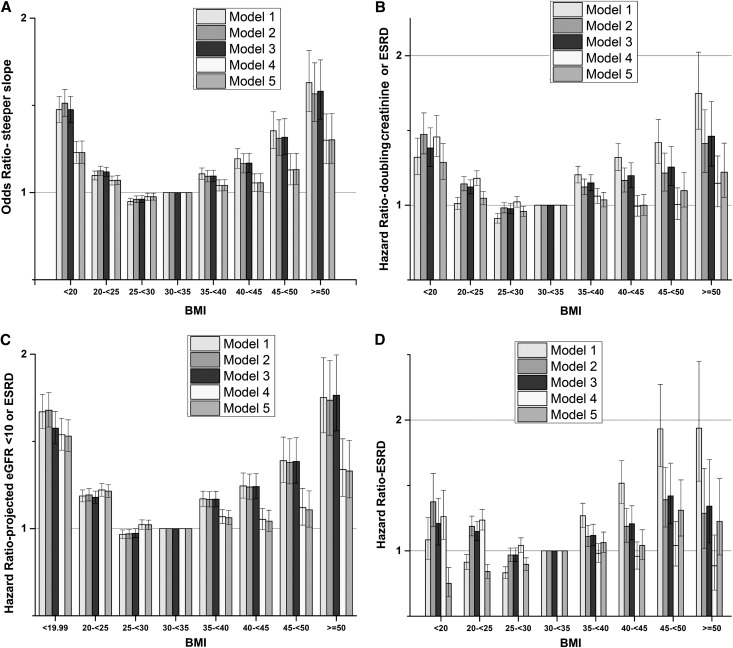
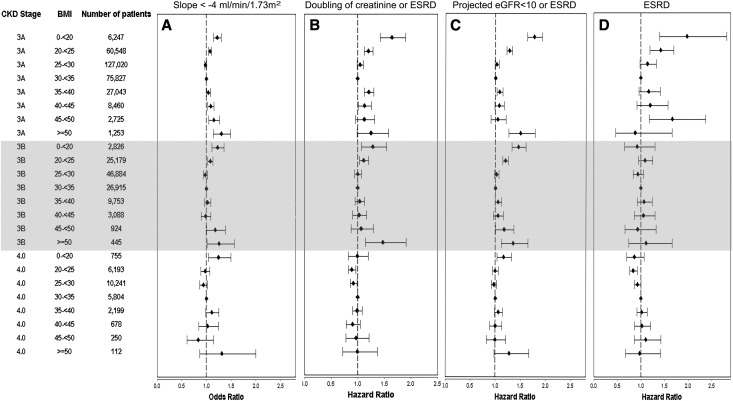
Obesity is associated with higher mortality in the general population, but this association is reversed in patients on dialysis. The nature of the relationship of obesity with adverse clinical outcomes in nondialysis-dependent CKD and the putative interaction of the severity of disease with this association are unclear. We analyzed data from a nationally representative cohort of 453,946 United States veterans with eGFR<60 ml/min per 1.73 m(2). The associations of body mass index categories (<20, 20 to <25, 25 to <30, 30 to <35, 35 to <40, 40 to <45, 45 to <50, and ≥50 kg/m(2)) with all-cause mortality and disease progression (using multiple definitions, including incidence of ESRD, doubling of serum creatinine, and the slopes of eGFR) were examined in Cox proportional hazards models and logistic regression models. Multivariable adjustments were made for age, race, comorbidities and medications, and baseline eGFR. Body mass index showed a relatively consistent U-shaped association with clinical outcomes, with the best outcomes observed in overweight and mildly obese patients. Body mass index levels <25 kg/m(2) were associated with worse outcomes in all patients, independent of severity of CKD. Body mass index levels ≥35 kg/m(2) were associated with worse outcomes in patients with earlier stages of CKD, but this association was attenuated in those patients with eGFR<30 ml/min per 1.73 m(2). Thus, until clinical trials establish the ideal body mass index, a cautious approach to weight management is warranted in this patient population.
Copyright © 2014 by the American Society of Nephrology.
Figures
References
-
- Kannel WB, Feinleib M, McNamara PM, Garrison RJ, Castelli WP: An investigation of coronary heart disease in families. The Framingham offspring study. Am J Epidemiol 110: 281–290, 1979 - PubMed
-
- Calle EE, Thun MJ, Petrelli JM, Rodriguez C, Heath CW, Jr.: Body-mass index and mortality in a prospective cohort of U.S. adults. N Engl J Med 341: 1097–1105, 1999 - PubMed
-
- Cornoni-Huntley JC, Harris TB, Everett DF, Albanes D, Micozzi MS, Miles TP, Feldman JJ: An overview of body weight of older persons, including the impact on mortality. The National Health and Nutrition Examination Survey I—Epidemiologic Follow-up Study. J Clin Epidemiol 44: 743–753, 1991 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
