

Fluorescence microangiography for quantitative assessment of peritubular capillary changes after AKI in mice
- PMID: 24652794
- PMCID: PMC4147987
- DOI: 10.1681/ASN.2013101121
Fluorescence microangiography for quantitative assessment of peritubular capillary changes after AKI in mice
Abstract
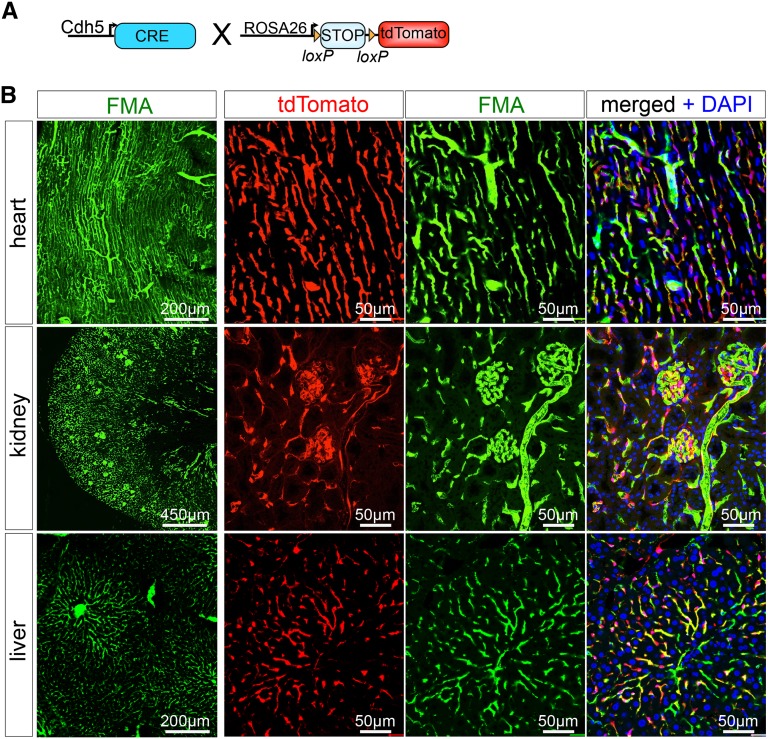
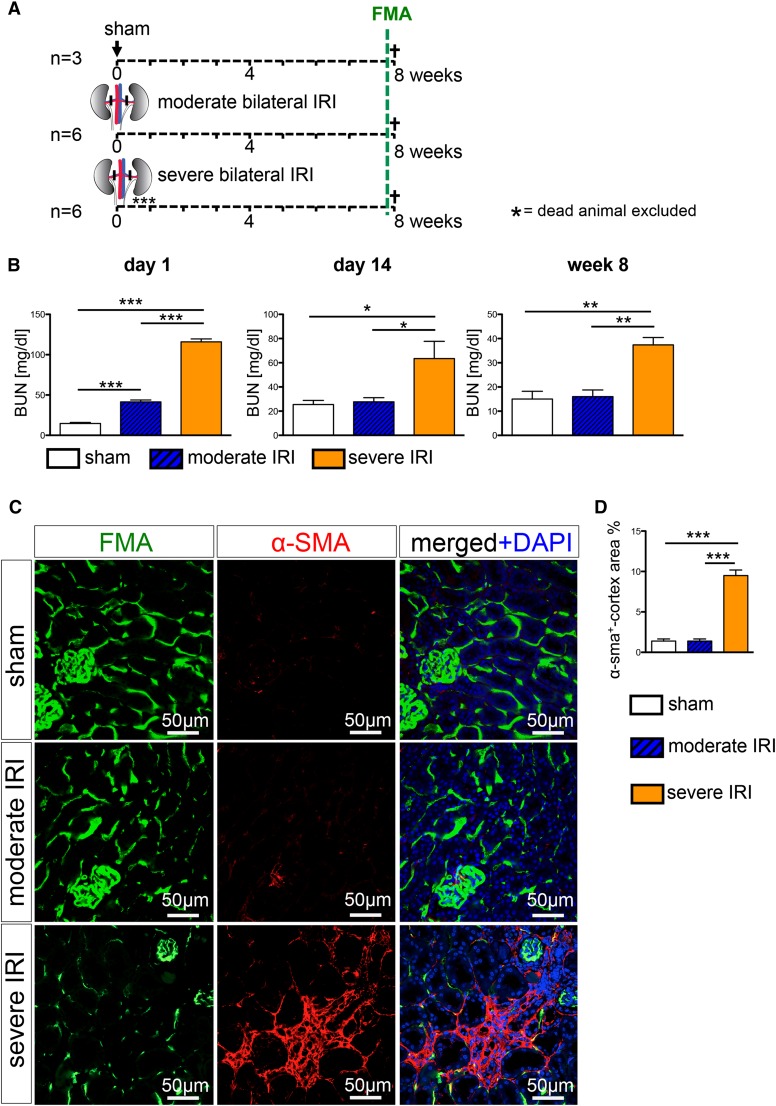
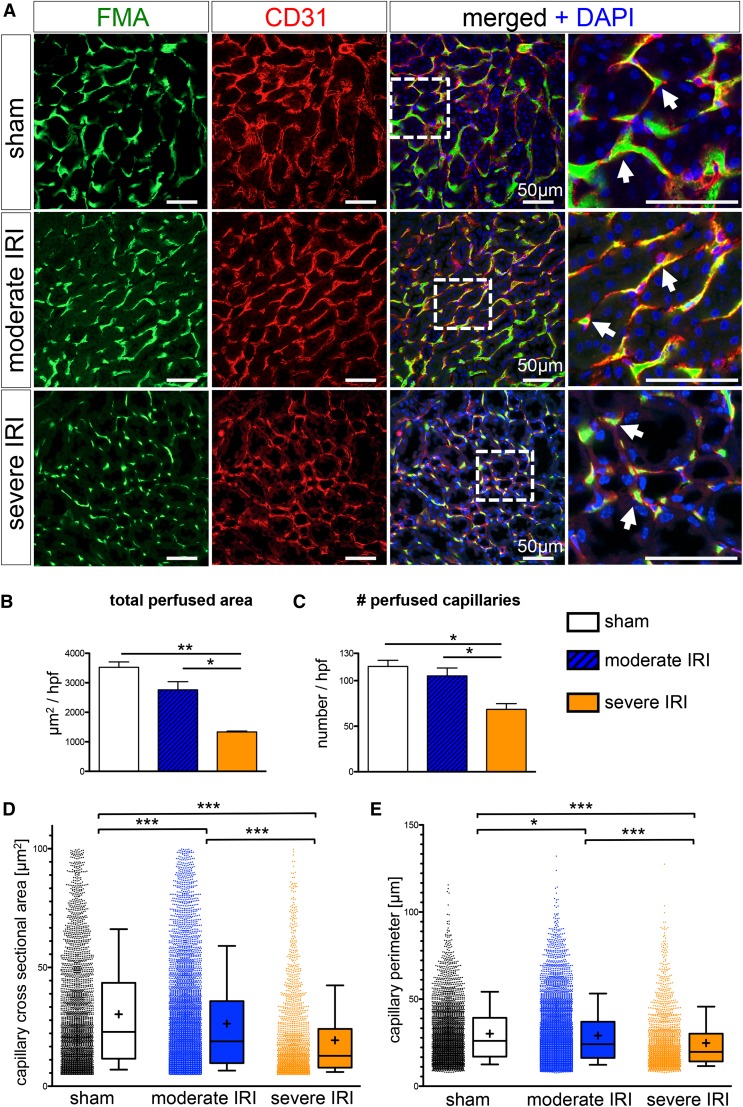
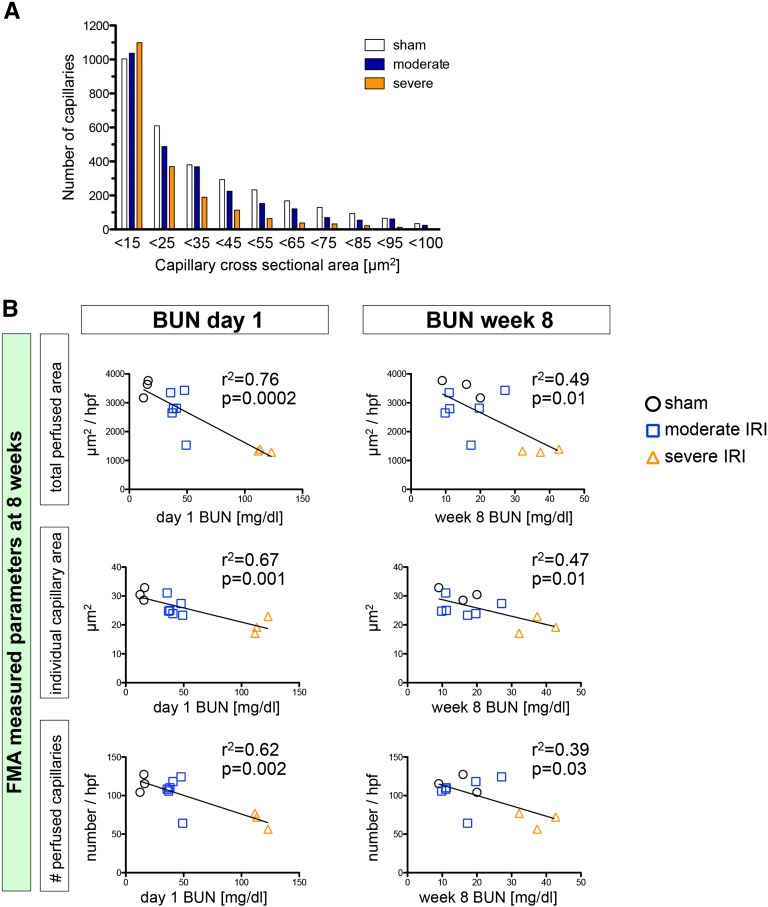
AKI predicts the future development of CKD, and one proposed mechanism for this epidemiologic link is loss of peritubular capillaries triggering chronic hypoxia. A precise definition of changes in peritubular perfusion would help test this hypothesis by more accurately correlating these changes with future loss of kidney function. Here, we have adapted and validated a fluorescence microangiography approach for use with mice to visualize, analyze, and quantitate peritubular capillary dynamics after AKI. A novel software-based approach enabled rapid and automated quantitation of capillary number, individual area, and perimeter. After validating perfusion in mice with genetically labeled endothelia, we compared peritubular capillary number and size after moderate AKI, characterized by complete renal recovery, and after severe AKI, characterized by development of interstitial fibrosis and CKD. Eight weeks after severe AKI, we measured a 40%±7.4% reduction in peritubular capillary number (P<0.05) and a 36%±4% decrease in individual capillary cross-sectional area (P<0.001) for a 62%±2.2% reduction in total peritubular perfusion (P<0.01). Whereas total peritubular perfusion and number of capillaries did not change, we detected a significant change of single capillary size following moderate AKI. The loss of peritubular capillary density and caliber at week 8 closely correlated with severity of kidney injury at day 1, suggesting irreparable microvascular damage. These findings emphasize a direct link between severity of acute injury and future loss of peritubular perfusion, demonstrate that reduced capillary caliber is an unappreciated long-term consequence of AKI, and offer a new quantitative imaging tool for understanding how AKI leads to future CKD in mouse models.
Keywords: acute renal failure; chronic kidney disease; vascular disease.
Copyright © 2014 by the American Society of Nephrology.
Figures
References
-
- Chawla LS, Kimmel PL: Acute kidney injury and chronic kidney disease: An integrated clinical syndrome. Kidney Int 82: 516–524, 2012 - PubMed
-
- Humphreys BD, Valerius MT, Kobayashi A, Mugford JW, Soeung S, Duffield JS, McMahon AP, Bonventre JV: Intrinsic epithelial cells repair the kidney after injury. Cell Stem Cell 2: 284–291, 2008 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
