

Telaprevir or boceprevir triple therapy in patients with chronic hepatitis C and varying severity of cirrhosis
- PMID: 24654657
- PMCID: PMC4385588
- DOI: 10.1111/apt.12718
Telaprevir or boceprevir triple therapy in patients with chronic hepatitis C and varying severity of cirrhosis
Abstract
Background: Risks and benefits of protease inhibitor (PI) (telaprevir or boceprevir) triple therapy in hepatitis C virus (HCV)-infected patients with mildly decompensated cirrhosis, including those wait-listed for liver transplantation (LT), are incompletely known.
Aim: To assess virological responses and safety of PI triple therapy in patients with mildly decompensated Child-Pugh (CP) CP ≥6 vs. compensated (CP = 5) cirrhosis.
Methods: Multicentre cohort of 160 adults with cirrhosis treated with peginterferon/ribavirin (peg-IFN/RBV) plus telaprevir (69%) or boceprevir (31%), comparing outcomes between those with CP = 5 and CP ≥6.
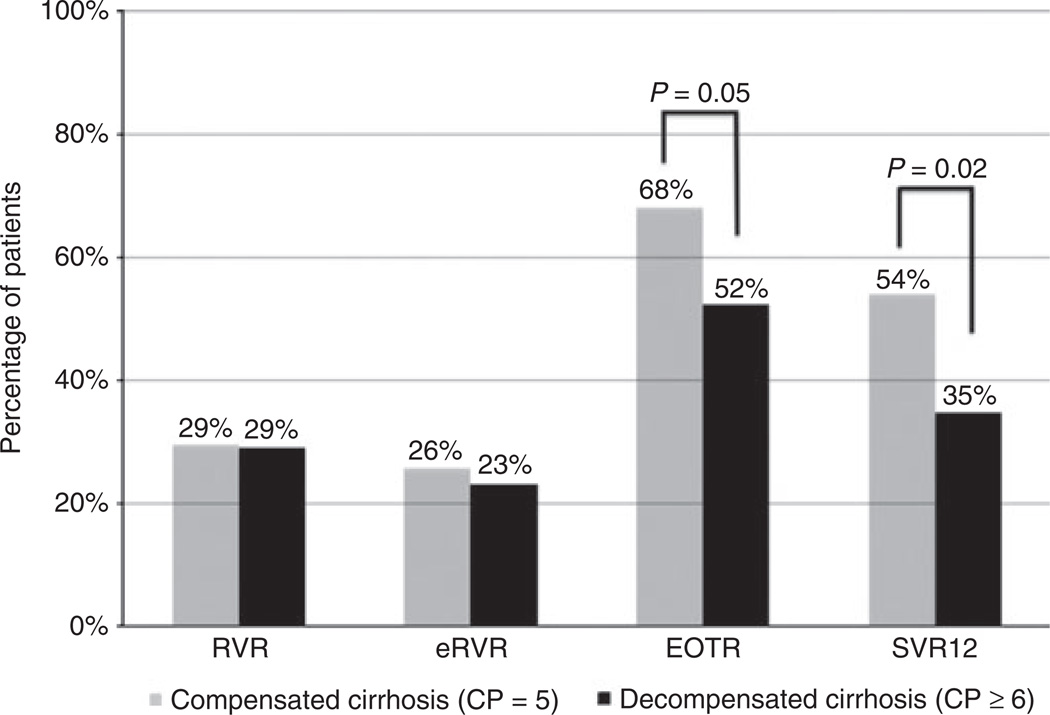
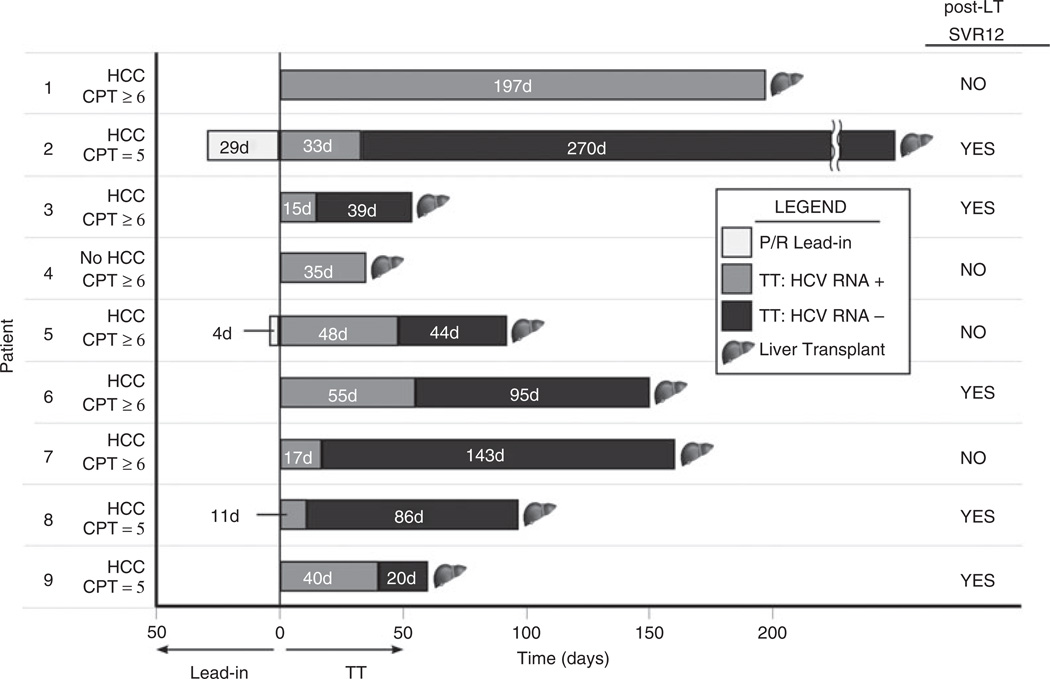
Results: Patients, 47% with CP ≥6 cirrhosis (CP range 6-10), received PI triple therapy for a targeted duration of 48 weeks. The cohort was median age 59 years, 32% female, 59% genotype 1a, 35% previous null/partial responders. Sustained virological response at 12 weeks (SVR12) was achieved by 35% of patients with CP ≥6 vs. 54% of those with CP = 5 (P = 0.02). CP = 5, achievement of rapid virological response and genotype 1b/other, independently predicted SVR12. Compared to those with CP = 5, patients with CP ≥6 had more peg-IFN dose reductions, eltrombopag use, transfusions and hospitalisations to manage adverse events (all P < 0.05). Overall, 67 (42%) discontinued treatment early. Nine wait-listed patients were treated for a median of 97 days (IQR 60-160) prior to liver transplantation and five achieved post-LT SVR.
Conclusions: In the presence of mild decompensation (Child-Pugh ≥6), SVR12 rates with protease inhibitor triple therapy are significantly reduced and adverse events increased. Thus, treatment with protease inhibitor triple therapy, if judged as necessary, should be undertaken with close monitoring and awareness of the significant risks.
© 2014 John Wiley & Sons Ltd.
Figures
Comment in
-
Commentary: treatment of hepatitis C-related cirrhosis in the era of direct-acting anti-virals.Aliment Pharmacol Ther. 2014 Jun;39(12):1427-8. doi: 10.1111/apt.12745. Aliment Pharmacol Ther. 2014. PMID: 24849149 No abstract available.
-
Commentary: treatment of hepatitis C-related cirrhosis in the era of direct-acting anti-virals - authors' reply.Aliment Pharmacol Ther. 2014 Jun;39(12):1428. doi: 10.1111/apt.12775. Aliment Pharmacol Ther. 2014. PMID: 24849150 No abstract available.
References
-
- Armstrong GL, Wasley A, Simard EP, McQuillan GM, Kuhnert WL, Alter MJ. The prevalence of hepatitis C virus infection in the United States, 1999 through 2002. Ann Intern Med. 2006;144:705–714. - PubMed
-
- Alter MJ, Hadler SC, Judson FN, et al. Risk factors for acute non-A, non-B hepatitis in the United States and association with hepatitis C virus infection. JAMA. 1990;264:2231–2235. - PubMed
-
- Davis GL, Albright JE, Cook SF, Rosenberg DM. Projecting future complications of chronic hepatitis C in the United States. Liver Transpl. 2003;9:331–338. - PubMed
-
- van der Meer AJ, Veldt BJ, Feld JJ, et al. Association between sustained virological response and all-cause mortality among patients with chronic hepatitis C and advanced hepatic fibrosis. JAMA. 2012;308:2584–2593. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous