

The diversity of young adult wheeze: a cluster analysis in a longitudinal birth cohort
- PMID: 24654674
- PMCID: PMC4010938
- DOI: 10.1111/cea.12306
The diversity of young adult wheeze: a cluster analysis in a longitudinal birth cohort
Abstract
Background: Cluster analyses have enhanced understanding of the heterogeneity of both paediatric and adult wheezing. However, while adolescence represents an important transitional phase, the nature of young adult wheeze has yet to be clearly characterised.
Objectives: To use cluster analysis to define, for the first time, clinically relevant young adult wheeze clusters in a longitudinal birth cohort.
Methods: K-means cluster analysis was undertaken among 309 currently wheezing subjects at 18 years in the Isle of Wight birth cohort (N = 1456). Thirteen disease-characterising clustering variables at 18 years were used. Resulting clusters were then further characterised by severity indices plus potential risk factors for wheeze development throughout the 1st 18 years of life.
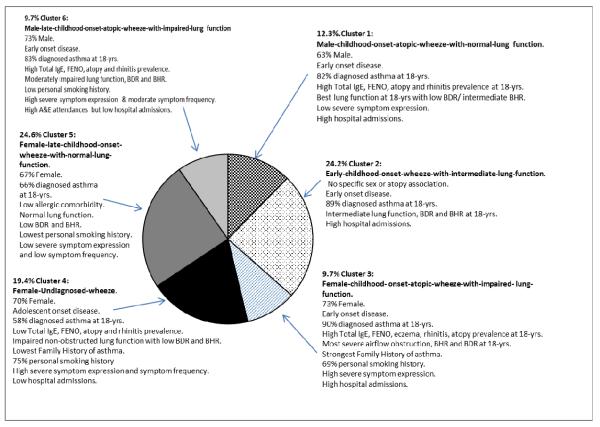
Results: Six wheeze clusters were identified. Cluster 1 (12.3%) male-early-childhood-onset-atopic-wheeze-with-normal-lung-function had male predominance, normal spirometry, low bronchodilator reversibility (BDR), intermediate bronchial hyper-responsiveness (BHR), high atopy prevalence and more admissions. Cluster 2 (24.2%) early-childhood-onset-wheeze-with-intermediate-lung-function had no specific sex association, intermediate spirometry, BDR, BHR, more significant BTS step therapy and admissions. Cluster 3 (9.7%) female-early-childhood-onset-atopic-wheeze-with-impaired-lung-function showed female predominance, high allergic disease comorbidity, more severe BDR and BHR, greatest airflow obstruction, high smoking prevalence, higher symptom severity and admissions. Cluster 4 (19.4%) female-undiagnosed-wheezers had adolescent-onset non-atopic wheeze, low BDR and BHR, impaired but non-obstructed spirometry, high symptom frequency and highest smoking prevalence. Cluster 5 (24.6%) female-late-childhood-onset-wheeze-with-normal-lung-function showed no specific atopy association, normal spirometry, low BDR, BHR and symptom severity. Cluster 6 (9.7%) male-late-childhood-onset-atopic-wheeze-with-impaired-lung-function had high atopy and rhinitis prevalence, increased BDR and BHR, moderately impaired spirometry, high symptom severity and higher BTS step therapy.
Conclusions and clinical relevance: Young adult wheeze is diverse and can be classified into distinct clusters. More severe clusters merit attention and are associated with childhood onset, atopy, impaired lung function and in some, smoking. Smoking-associated undiagnosed wheezers also merit recognition. Better understanding of young adult wheeze could facilitate better later adult respiratory health.
Keywords: asthma; cluster analysis; morbidity; severity; smoking; wheeze.
© 2014 John Wiley & Sons Ltd.
Figures

References
-
- Braman SS. The global burden of asthma. Chest. 2006;130(1 Suppl):4S–12S. - PubMed
-
- Borish L, Culp JA. Asthma: a syndrome composed of heterogeneous diseases. Ann Allergy Asthma Immunol. 2008 Jul;101(1):1–8. - PubMed
-
- Fitzpatrick AM, Teague WG, Meyers DA, Peters SP, Li X, Li H, Wenzel SE, Aujla S, Castro M, Bacharier LB, Gaston BM, Bleecker ER, Moore WC, National Institutes of Health/National Heart, Lung, and Blood Institute Severe Asthma Research Program Heterogeneity of severe asthma in childhood: confirmation by cluster analysis of children in the National Institutes of Health/National Heart, Lung, and Blood Institute Severe Asthma Research Program. J Allergy Clin Immunol. 2011 Feb;127(2):382–389. e1–13. - PMC - PubMed
-
- Just J, Gouvis-Echraghi R, Rouve S, Wanin S, Moreau D, Annesi Maesano I. Two novel severe asthma phenotypes identified during childhood using a clustering approach. Eur Respir J. 2012;40:55–60. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
