

The clinical and molecular epidemiology of Staphylococcus aureus infections in Fiji
- PMID: 24655406
- PMCID: PMC3998116
- DOI: 10.1186/1471-2334-14-160
The clinical and molecular epidemiology of Staphylococcus aureus infections in Fiji
Abstract
Background: There are few data describing the microbiology and genetic typing of Staphylococcus aureus that cause infections in developing countries.
Methods: In this study we observed S. aureus infections in Pacific Island nation of Fiji in both the community and hospital setting with an emphasis on clonal complex (CC) genotyping and antimicrobial susceptibility.
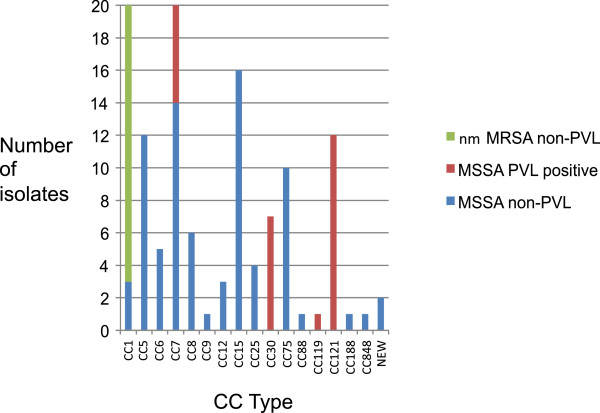
Results: S. aureus was commonly found in impetigo lesions of school children and was recovered from 57% of impetigo lesions frequently in conjunction with group A streptococcal infection. Methicillin-resistant S. aureus (MRSA) comprised 7% (20/299) of isolates and were all non-multi-resistant and all genotyped as CC1. In contrast, there was a diverse selection of 17 CCs among the 105 genotyped methicillin-susceptible S.aureus (MSSA) strains. Isolates of the rare, phylogenetically divergent and non-pigmented CC75 lineage (also called S. argenteus) were found in Fiji.From hospitalized patients the available 36 MRSA isolates from a 9-month period were represented by five CCs. The most common CCs were CC1 and CC239. CC1 is likely to be a community-acquired strain, reflecting what was found in the school children, whereas the CC239 is the very successful multi-drug resistant MRSA nosocomial lineage. Of 17 MSSA isolates, 59% carried genes for Panton-Valentine leukocidin. The S. aureus bacteraemia incidence rate of 50 per 100,000 population is among the highest reported in the literature and likely reflects the high overall burden of staphylococcal infections in this population.
Conclusions: S. aureus is an important cause of disease in Fiji and there is considerable genotypic diversity in community skin infections in Fijian schoolchildren. Community acquired- (CA)- MRSA is present at a relatively low prevalence (6.7%) and was solely to CC1 (CA-MRSA). The globally successful CC239 is also a significant pathogen in Fiji.
Figures


References
-
- Allegranzi B, Bagheri Nejad S, Combescure C, Graafmans W, Attar H, Donaldson L, Pittet D. Burden of endemic health-care-associated infection in developing countries: systematic review and meta-analysis. Lancet. pp. 228–241. - PubMed
-
- Nickerson EK, Wuthiekanun V, Wongsuvan G, Limmathurosakul D, Srisamang P, Mahavanakul W, Thaipadungpanit J, Shah KR, Arayawichanont A, Amornchai P, Thanwisai A, Day NP, Peacock SJ. Factors predicting and reducing mortality in patients with invasive staphylococcus aureus disease in a developing country. PLoS One. 2009;14(8):e6512. doi: 10.1371/journal.pone.0006512. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
