

A cross-sectional study of determinants of indoor environmental exposures in households with and without chronic exposure to biomass fuel smoke
- PMID: 24655424
- PMCID: PMC3978088
- DOI: 10.1186/1476-069X-13-21
A cross-sectional study of determinants of indoor environmental exposures in households with and without chronic exposure to biomass fuel smoke
Abstract
Background: Burning biomass fuels indoors for cooking is associated with high concentrations of particulate matter (PM) and carbon monoxide (CO). More efficient biomass-burning stoves and chimneys for ventilation have been proposed as solutions to reduce indoor pollution. We sought to quantify indoor PM and CO exposures in urban and rural households and determine factors associated with higher exposures. A secondary objective was to identify chronic vs. acute changes in cardiopulmonary biomarkers associated with exposure to biomass smoke.
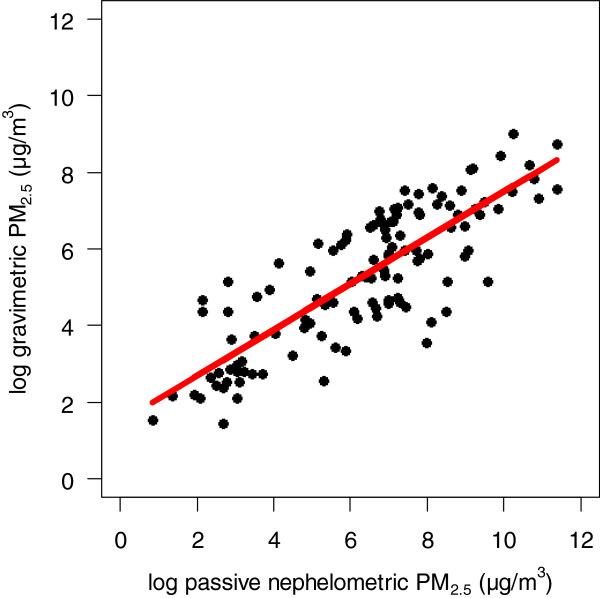
Methods: We conducted a census survey followed by a cross-sectional study of indoor environmental exposures and cardiopulmonary biomarkers in the main household cook in Puno, Peru. We measured 24-hour indoor PM and CO concentrations in 86 households. We also measured PM2.5 and PM10 concentrations gravimetrically for 24 hours in urban households and during cook times in rural households, and generated a calibration equation using PM2.5 measurements.
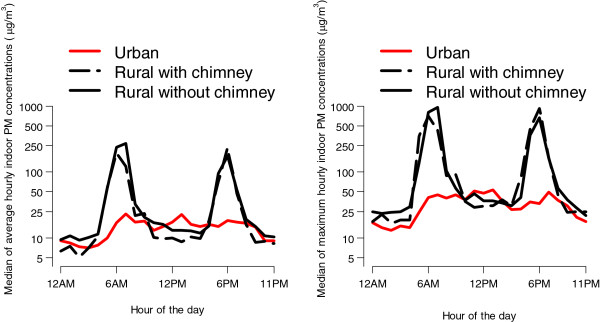
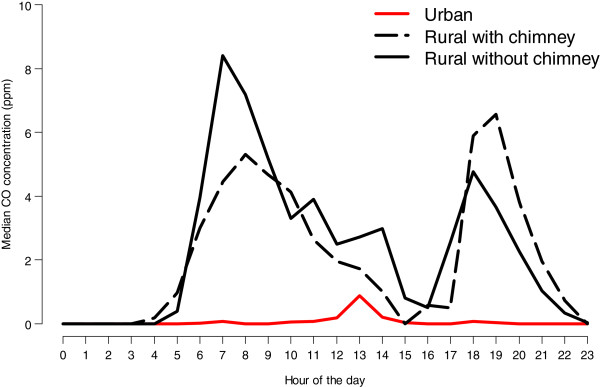
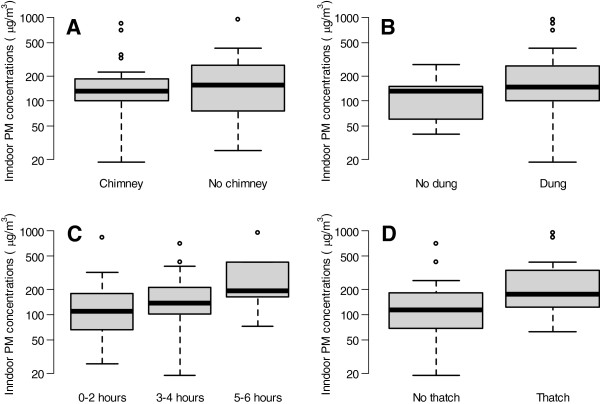
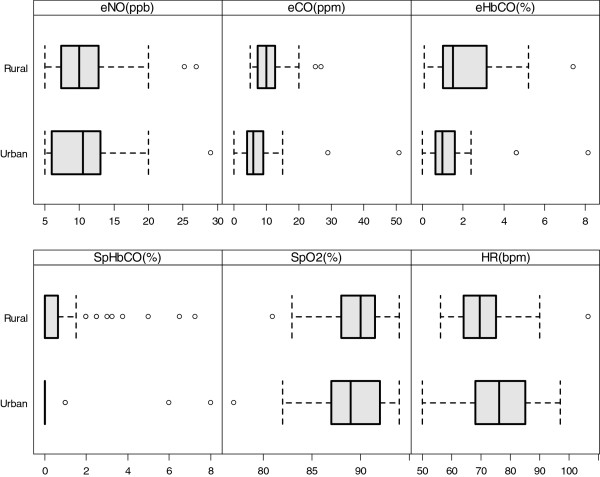
Results: In a census of 4903 households, 93% vs. 16% of rural vs. urban households used an open-fire stove; 22% of rural households had a homemade chimney; and <3% of rural households participated in a national program encouraging installation of a chimney. Median 24-hour indoor PM2.5 and CO concentrations were 130 vs. 22 μg/m3 and 5.8 vs. 0.4 ppm (all p<0.001) in rural vs. urban households. Having a chimney did not significantly reduce median concentrations in 24-hour indoor PM2.5 (119 vs. 137 μg/m3; p=0.40) or CO (4.6 vs. 7.2 ppm; p=0.23) among rural households with and without chimneys. Having a chimney did not significantly reduce median cook-time PM2.5 (360 vs. 298 μg/m3, p=0.45) or cook-time CO concentrations (15.2 vs. 9.4 ppm, p=0.23). Having a thatched roof (p=0.007) and hours spent cooking (p=0.02) were associated with higher 24-hour average PM concentrations. Rural participants had higher median exhaled CO (10 vs. 6 ppm; p=0.01) and exhaled carboxyhemoglobin (1.6% vs. 1.0%; p=0.04) than urban participants.
Conclusions: Indoor air concentrations associated with biomass smoke were six-fold greater in rural vs. urban households. Having a homemade chimney did not reduce environmental exposures significantly. Measures of exhaled CO provide useful cardiopulmonary biomarkers for chronic exposure to biomass smoke.
Figures
References
-
- Torres-Duque C, Maldonado D, Pérez-Padilla R, Ezzati M, Viegi G. Forum of International Respiratory Studies (FIRS) Task Force on Health Effects of Biomass Exposure. Biomass fuels and respiratory diseases: a review of the evidence. Proc Am Thorac Soc. 2008;5:577–590. doi: 10.1513/pats.200707-100RP. - DOI - PubMed
-
- Mathers C, Stevens G, Mascarenhas M. Global health risks: mortality and burden of disease attributable to selected major risks. Geneva: World Health Organization; 2009.
-
- Lim SS, Vos T, Flaxman AD, Danaei G, Shibuya K, Adair-Rohani H, Amann M, Anderson HR, Andrews KG, Aryee M, Atkinson C, Bacchus LJ, Bahalim AN, Balakrishnan K, Balmes J, Barker-Collo S, Baxter A, Bell ML, Blore JD, Blyth F, Bonner C, Borges G, Bourne R, Boussinesq M, Brauer M, Brooks P, Bruce NG, Brunekreef B, Bryan-Hancock C, Bucello C. et al.A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2224–2260. doi: 10.1016/S0140-6736(12)61766-8. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
