

Unintended effects of statins from observational studies in the general population: systematic review and meta-analysis
- PMID: 24655568
- PMCID: PMC3998050
- DOI: 10.1186/1741-7015-12-51
Unintended effects of statins from observational studies in the general population: systematic review and meta-analysis
Abstract
Background: Efficacy of statins has been extensively studied, with much less information reported on their unintended effects. Evidence from randomized controlled trials (RCTs) on unintended effects is often insufficient to support hypotheses generated from observational studies. We aimed to systematically assess unintended effects of statins from observational studies in general populations with comparison of the findings where possible with those derived from randomized trials.
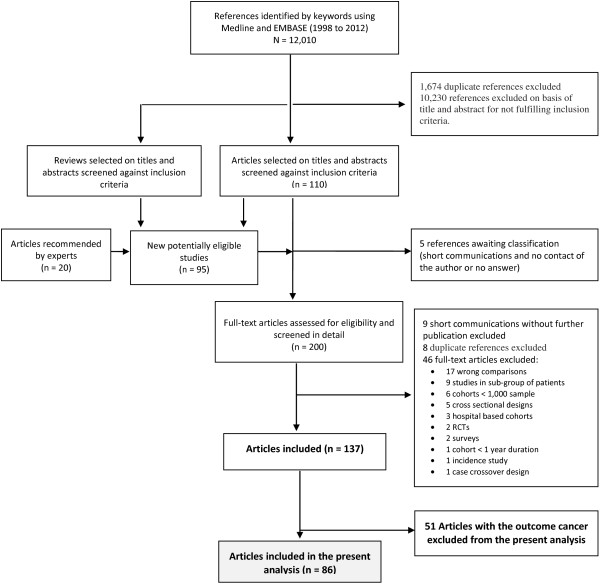
Methods: Medline (1998 to January 2012, week 3) and Embase (1998 to 2012, week 6) were searched using the standard BMJ Cohort studies filter. The search was supplemented with reference lists of all identified studies and contact with experts in the field. We included prospective studies with a sample size larger than 1,000 participants, case control (of any size) and routine health service linkage studies of over at least one year duration. Studies in subgroups of patients or follow-up of patient case series were excluded, as well as hospital-based cohort studies.
Results: Ninety studies were identified, reporting on 48 different unintended effects. Statins were associated with lower risks of dementia and cognitive impairment, venous thrombo-embolism, fractures and pneumonia, but these findings were attenuated in analyses restricted to higher quality studies (respectively: OR 0.74 (95% CI 0.62 to 0.87); OR 0.92 (95% CI 0.81 to 1.03); OR 0.97 (95% CI 0.88 to 1.05); OR 0.92 (95% CI 0.83 to 1.02)); and marked heterogeneity of effects across studies remained. Statin use was not related to any increased risk of depression, common eye diseases, renal disorders or arthritis. There was evidence of an increased risk of myopathy, raised liver enzymes and diabetes (respectively: OR 2.63 (95% CI 1.50 to 4.61); OR 1.54 (95% CI 1.47 to 1.62); OR 1.31 (95% CI 0.99 to 1.73)).
Conclusions: Our systematic review and meta-analyses indicate that high quality observational data can provide relevant evidence on unintended effects of statins to add to the evidence from RCTs. The absolute excess risk of the observed harmful unintended effects of statins is very small compared to the beneficial effects of statins on major cardiovascular events.
Figures


References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
