

Transperitoneal approach versus retroperitoneal approach: a meta-analysis of laparoscopic partial nephrectomy for renal cell carcinoma
- PMID: 24658032
- PMCID: PMC3962363
- DOI: 10.1371/journal.pone.0091978
Transperitoneal approach versus retroperitoneal approach: a meta-analysis of laparoscopic partial nephrectomy for renal cell carcinoma
Abstract
Objective: To compare the efficiency and safety of the transperitoneal approaches with retroperitoneal approaches in laparoscopic partial nephrectomy for renal cell carcinoma and provide evidence-based medicine support for clinical treatment.
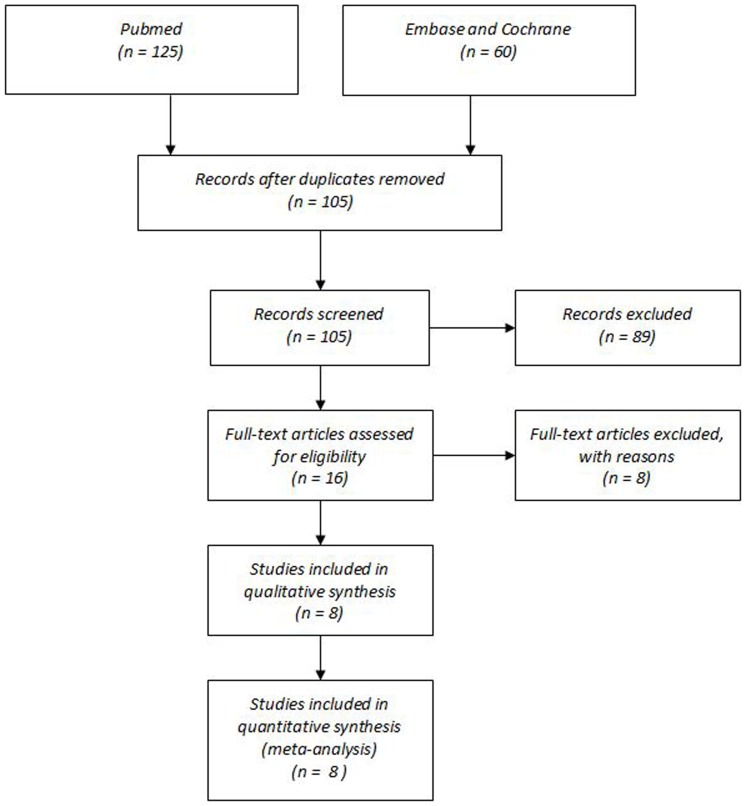
Methods: A systematic computer search of PUBMED, EMBASE, and the Cochrane Library was executed to identify retrospective observational and prospective randomized controlled trials studies that compared the outcomes of the two approaches in laparoscopic partial nephrectomy. Two reviewers independently screened, extracted, and evaluated the included studies and executed statistical analysis by using software STATA 12.0. Outcomes of interest included perioperative and postoperative variables, surgical complications and oncological variables.
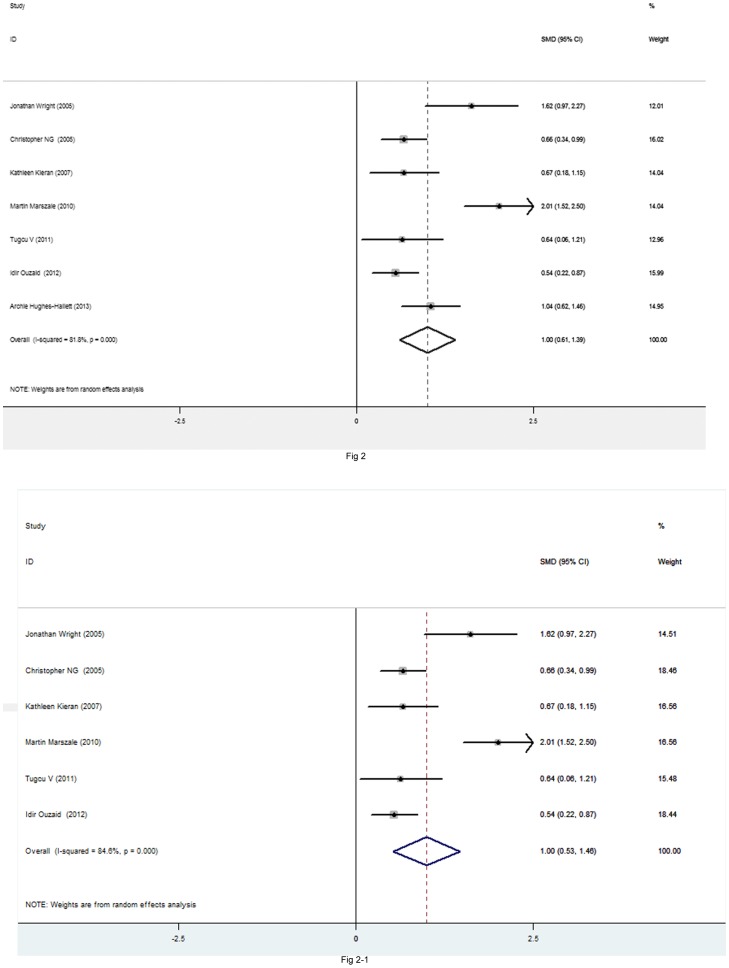
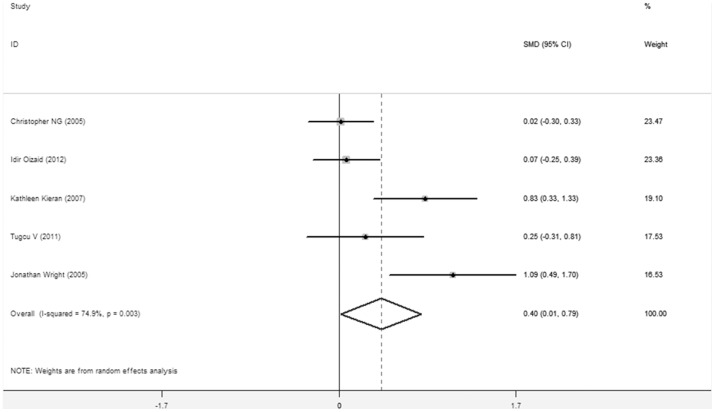
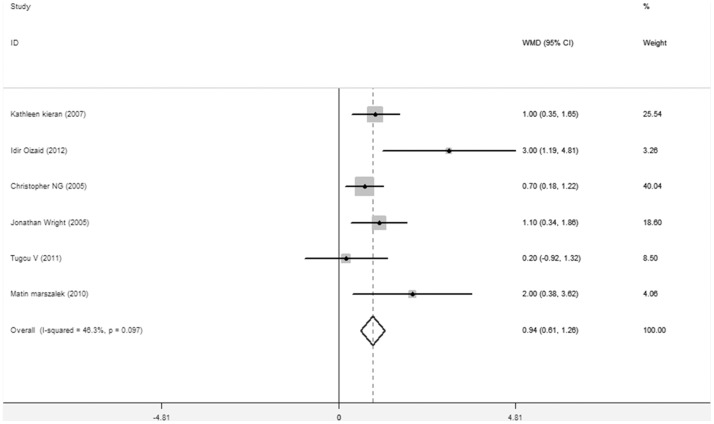
Results: There were 8 studies assessed transperitoneal laparoscopic partial nephrectomy (TLPN) versus retroperitoneal laparoscopic partial nephrectomy (RLPN) were included. RLPN had a shorter operating time (SMD = 1.001,95%confidence interval[CI] 0.609-1.393,P<0.001), a lower estimated blood loss (SMD = 0.403,95%CI 0.015-0.791,P = 0.042) and a shorter length of hospital stay (WMD = 0.936 DAYS,95%CI 0.609-1.263,P<0.001) than TLPN. There were no significant differences between the transperitoneal and retroperitoneal approaches in other outcomes of interest.
Conclusions: This meta-analysis indicates that, in appropriately selected patients, especially patients with intraperitoneal procedures history or posteriorly located renal tumors, the RLPN can shorten the operation time, reduce the estimated blood loss and shorten the length of hospital stay. RLPN may be equally safe and be faster compared with the TLPN.
Conflict of interest statement
Figures
References
-
- Ljungberg B, Cowan NC, Hanbury DC, Hora M, Merseburger AS, et al. (2010) EAU guidelines on renal cell carcinoma: the 2010 update. Eur Urol 58: 398–406. - PubMed
-
- Landis SH, Murray T, Bolden S, Wingo PA (1999) Cancer statistics, 1999. A Cancer Journal for Clinicians 49 (1): 8–31. - PubMed
-
- Mathew A, Devesa SS, Fraumeni JF Jr, Chow WH (2002) Global increases in kidney cancer incidence, 1973–1992. EurJCancerPrev 11: 171–8. - PubMed
-
- Allan JD, Tolley DA, Kaouk JH (2001) Laparoscopic radical nephrectomy. Eur Urol 40: 17–23. - PubMed
-
- Portis AJ, Elnady M, Clayman RV (2001) Laparoscopic radical/total nephrectomy: a decade of progress. J Endourol 15: 345–54 discussion 375–6. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
