

Recipient-related clinical risk factors for primary graft dysfunction after lung transplantation: a systematic review and meta-analysis
- PMID: 24658073
- PMCID: PMC3962459
- DOI: 10.1371/journal.pone.0092773
Recipient-related clinical risk factors for primary graft dysfunction after lung transplantation: a systematic review and meta-analysis
Abstract
Background: Primary graft dysfunction (PGD) is the main cause of early morbidity and mortality after lung transplantation. Previous studies have yielded conflicting results for PGD risk factors. Herein, we carried out a systematic review and meta-analysis of published literature to identify recipient-related clinical risk factors associated with PGD development.
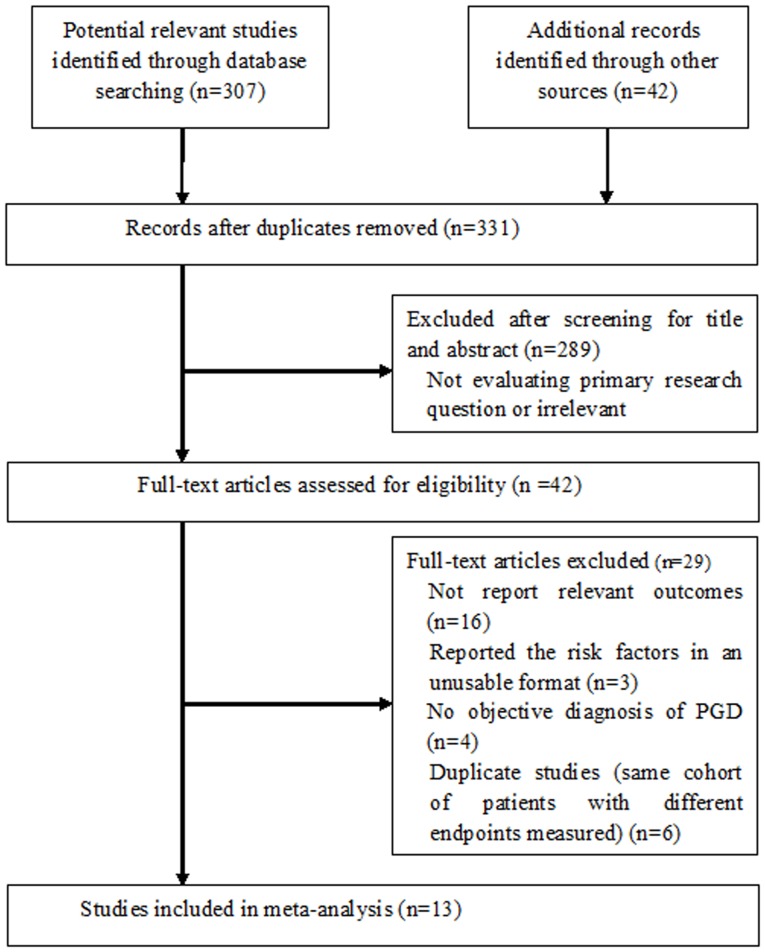
Method: A systematic search of electronic databases (PubMed, Embase, Web of Science, Cochrane CENTRAL, and Scopus) for studies published from 1970 to 2013 was performed. Cohort, case-control, or cross-sectional studies that examined recipient-related risk factors of PGD were included. The odds ratios (ORs) or mean differences (MDs) were calculated using random-effects models.
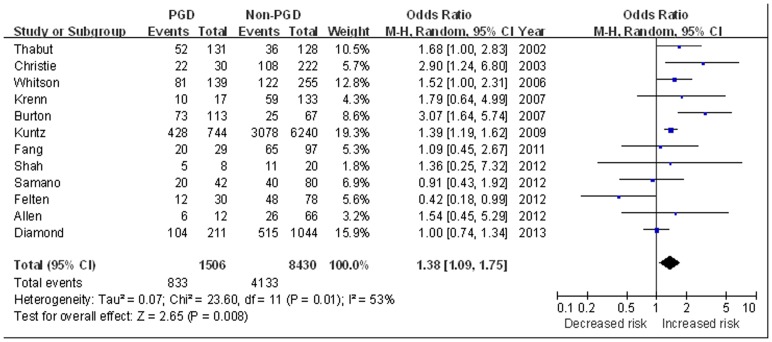
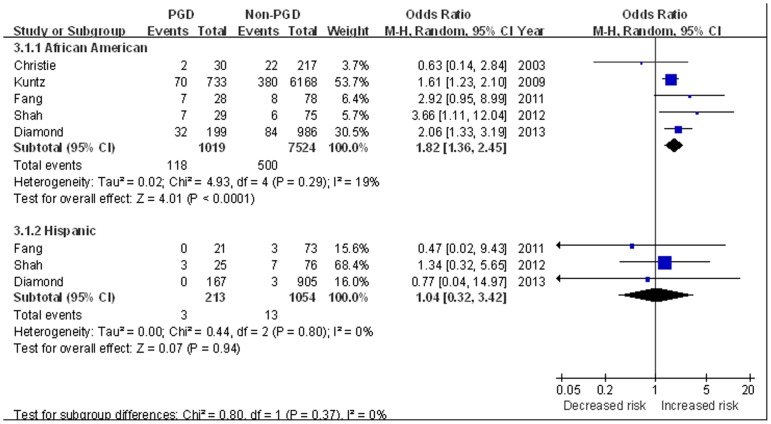
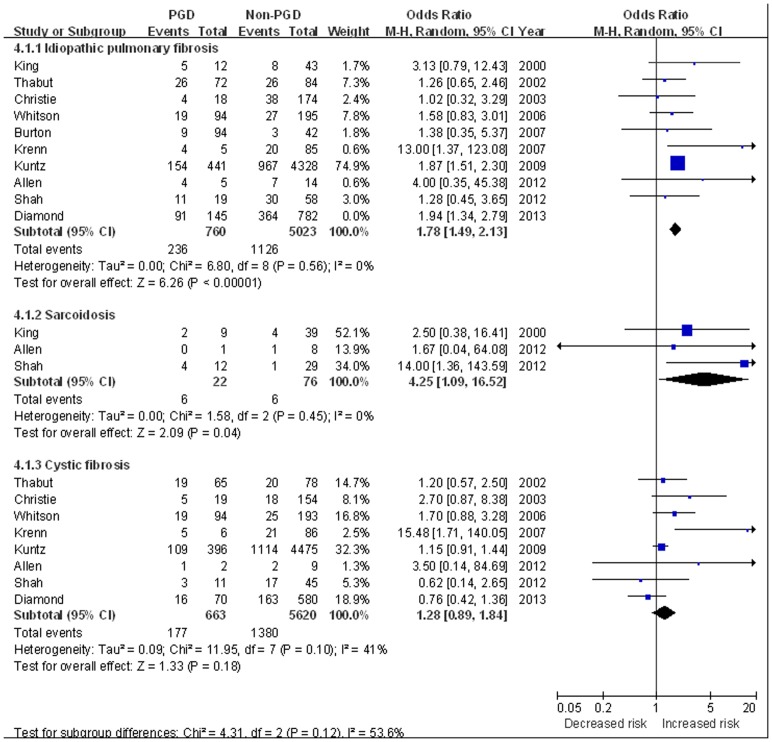
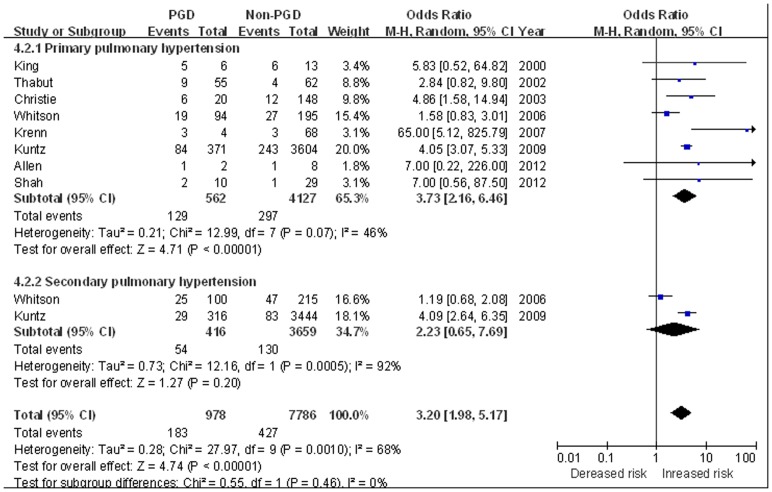
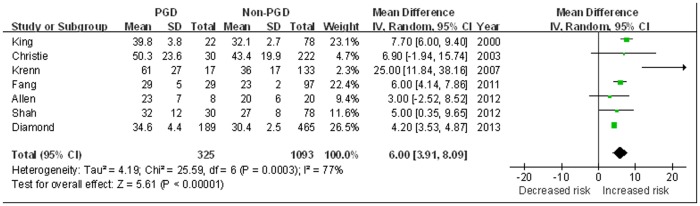
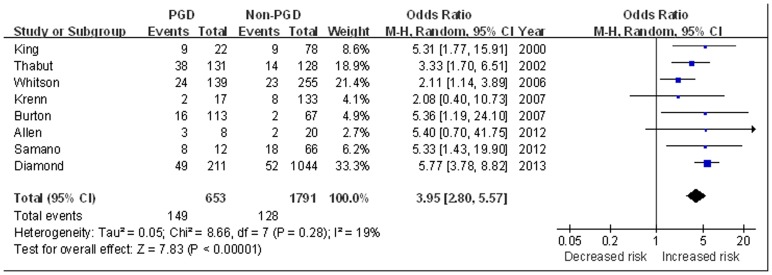
Result: Thirteen studies involving 10042 recipients met final inclusion criteria. From the pooled analyses, female gender (OR 1.38, 95% CI 1.09 to 1.75), African American (OR 1.82, 95%CI 1.36 to 2.45), idiopathic pulmonary fibrosis (IPF) (OR 1.78, 95% CI 1.49 to 2.13), sarcoidosis (OR 4.25, 95% CI 1.09 to 16.52), primary pulmonary hypertension (PPH) (OR 3.73, 95%CI 2.16 to 6.46), elevated BMI (BMI≥25 kg/m2) (OR 1.83, 95% CI 1.26 to 2.64), and use of cardiopulmonary bypass (CPB) (OR 2.29, 95%CI 1.43 to 3.65) were significantly associated with increased risk of PGD. Age, cystic fibrosis, secondary pulmonary hypertension (SPH), intra-operative inhaled nitric oxide (NO), or lung transplant type (single or bilateral) were not significantly associated with PGD development (all P>0.05). Moreover, a nearly 4 fold increased risk of short-term mortality was observed in patients with PGD (OR 3.95, 95% CI 2.80 to 5.57).
Conclusions: Our analysis identified several recipient related risk factors for development of PGD. The identification of higher-risk recipients and further research into the underlying mechanisms may lead to selective therapies aimed at reducing this reperfusion injury.
Conflict of interest statement
Figures
References
-
- Arcasoy SM, Kotloff RM (1999) Lung transplantation. N Engl J Med 340: 1081–1091. - PubMed
-
- Christie JD, Van Raemdonck D, de Perrot M, Barr M, Keshavjee S, et al. (2005) ISHLT Working Group on Primary Lung Graft Dysfunction (2005) Report of the ISHLT Working Group on Primary Lung Graft Dysfunction part I: introduction and methods. J Heart Lung Transplant 24: 1451–1453. - PubMed
-
- King RC, Binns OA, Rodriguez F, Kanithanon RC, Daniel TM, et al. (2000) Reperfusion injury significantly impacts clinical outcome after pulmonary transplantation. Ann Thorac Surg 69: 1681–1685. - PubMed
-
- Lee JC, Christie JD, Keshavjee S (2010) Primary graft dysfunction: definition, risk factors, short- and long-term outcomes. Semin Resp Crit Care Med 31: 161–71. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
