

The clinical relevance and management of monoclonal gammopathy of undetermined significance and related disorders: recommendations from the European Myeloma Network
- PMID: 24658815
- PMCID: PMC4040895
- DOI: 10.3324/haematol.2013.100552
The clinical relevance and management of monoclonal gammopathy of undetermined significance and related disorders: recommendations from the European Myeloma Network
Abstract
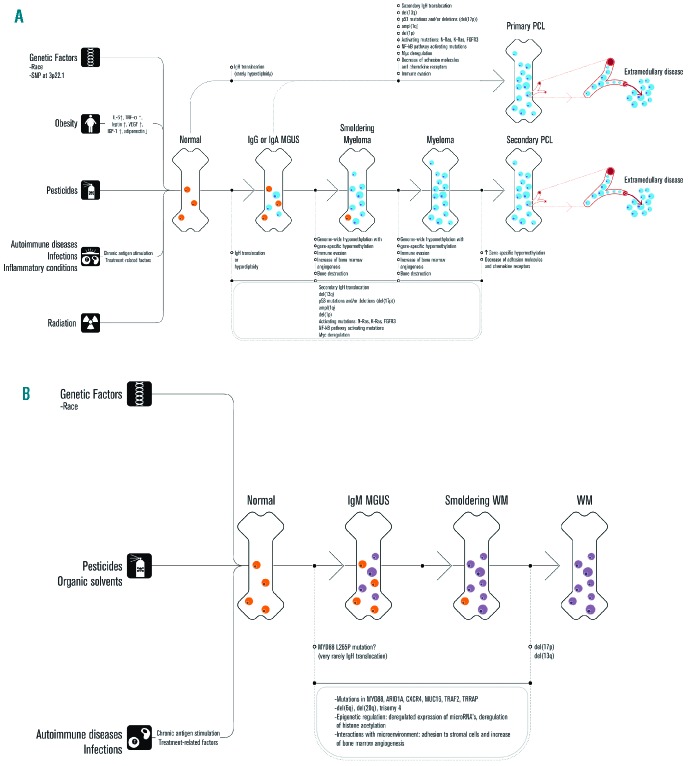
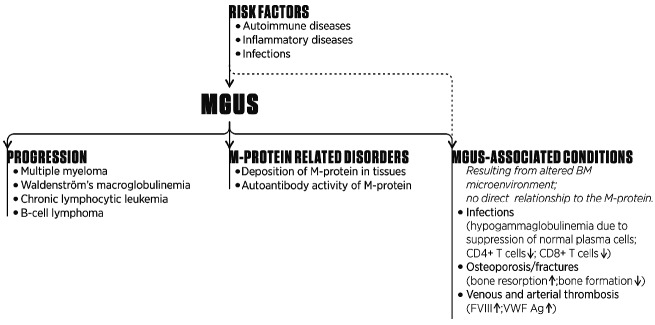
Monoclonal gammopathy of undetermined significance is one of the most common pre-malignant disorders. IgG and IgA monoclonal gammopathy of undetermined significance are precursor conditions of multiple myeloma; light-chain monoclonal gammopathy of undetermined significance of light-chain multiple myeloma; and IgM monoclonal gammopathy of undetermined significance of Waldenström's macroglobulinemia and other lymphoproliferative disorders. Clonal burden, as determined by bone marrow plasma cell percentage or M-protein level, as well as biological characteristics, including heavy chain isotype and light chain production, are helpful in predicting risk of progression of monoclonal gammopathy of undetermined significance to symptomatic disease. Furthermore, alterations in the bone marrow microenvironment of monoclonal gammopathy of undetermined significance patients result in an increased risk of venous and arterial thrombosis, infections, osteoporosis, and bone fractures. In addition, the small clone may occasionally be responsible for severe organ damage through the production of a monoclonal protein that has autoantibody activity or deposits in tissues. These disorders are rare and often require therapy directed at eradication of the underlying plasma cell or lymphoplasmacytic clone. In this review, we provide an overview of the clinical relevance of monoclonal gammopathy of undetermined significance. We also give general recommendations of how to diagnose and manage patients with monoclonal gammopathy of undetermined significance.
Copyright© Ferrata Storti Foundation.
Figures
References
-
- Eisele L, Durig J, Huttmann A, Duhrsen U, Assert R, Bokhof B, et al. Prevalence and progression of monoclonal gammopathy of undetermined significance and light-chain MGUS in Germany. Ann Hematol 2012; 91(2):243–8 - PubMed
-
- Kyle RA, Therneau TM, Rajkumar SV, Larson DR, Plevak MF, Offord JR, et al. Prevalence of monoclonal gammopathy of undetermined significance. N Engl J Med 2006;354(13):1362–9 - PubMed
-
- Kyle RA, Therneau TM, Rajkumar SV, Offord JR, Larson DR, Plevak MF, et al. A long-term study of prognosis in monoclonal gammopathy of undetermined significance. N Engl J Med 2002;346(8):564–9 - PubMed
-
- Owen RG, Treon SP, Al-Katib A, Fonseca R, Greipp PR, McMaster ML, et al. Clinicopathological definition of Waldenstrom’s macroglobulinemia: consensus panel recommendations from the Second International Workshop on Waldenstrom’s Macroglobulinemia. Semin Oncol 2003;30(2):110–5 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
