

Physiology and its importance for reference intervals
- PMID: 24659833
- PMCID: PMC3961997
Physiology and its importance for reference intervals
Abstract
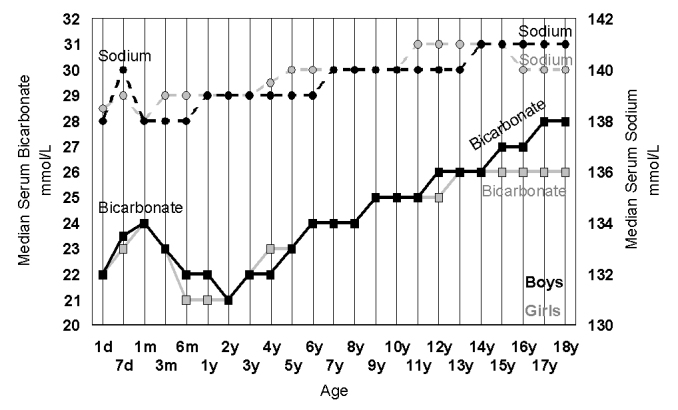
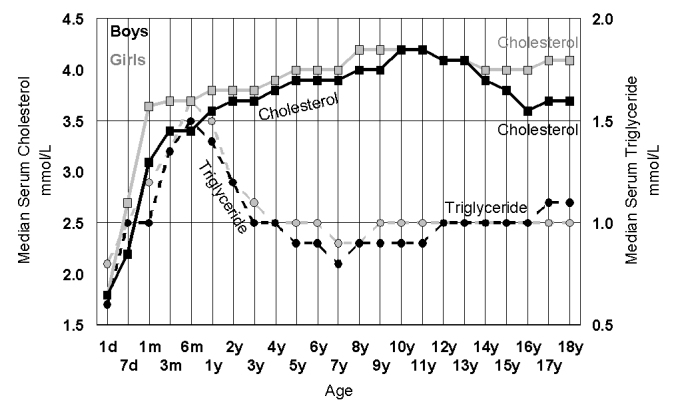
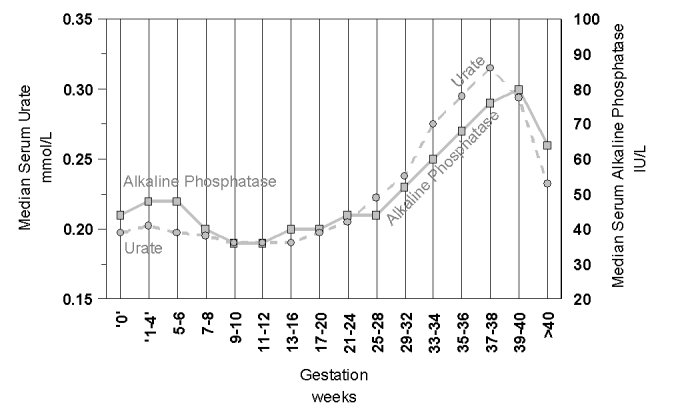
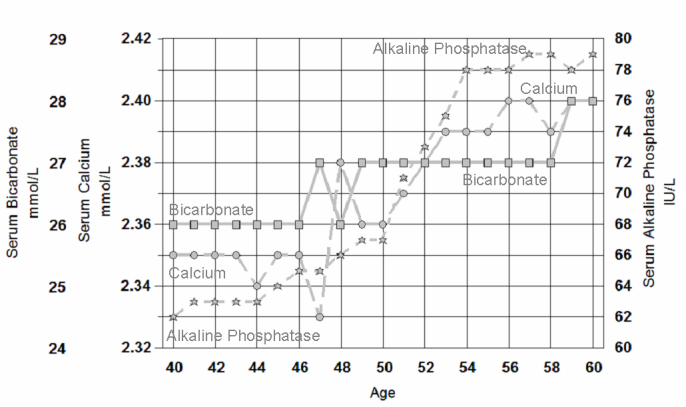
Reference intervals are ideally defined on apparently healthy individuals and should be distinguished from clinical decision limits that are derived from known diseased patients. Knowledge of physiological changes is a prerequisite for understanding and developing reference intervals. Reference intervals may differ for various subpopulations because of differences in their physiology, most obviously between men and women, but also in childhood, pregnancy and the elderly. Changes in laboratory measurements may be due to various physiological factors starting at birth including weaning, the active toddler, immunological learning, puberty, pregnancy, menopause and ageing. The need to partition reference intervals is required when there are significant physiological changes that need to be recognised. It is important that laboratorians are aware of these changes otherwise reference intervals that attempt to cover a widened inter-individual variability may lose their usefulness. It is virtually impossible for any laboratory to directly develop reference intervals for each of the physiological changes that are currently known, however indirect techniques can be used to develop or validate reference intervals in some difficult situations such as those for children. Physiology describes our life's journey, and it is only when we are familiar with that journey that we can appreciate a pathological departure.
Figures

References
-
- Lindstedt G, Tryding N. [There is difference between decision limits and reference intervals. Reference intervals are based on measurements in healthy individuals, decision limits on measurements in patients] Lakartidningen. 2007;104:2076–9. - PubMed
-
- Petersen PH, Jensen EA, Brandslund I. Analytical performance, reference values and decision limits. A need to differentiate between reference intervals and decision limits and to define analytical quality specifications. Clin Chem Lab Med. 2012;50:819–31. - PubMed
Publication types
LinkOut - more resources
Full Text Sources