

Histopathological evaluation of recurrent hepatitis C after liver transplantation: a review
- PMID: 24659874
- PMCID: PMC3961976
- DOI: 10.3748/wjg.v20.i11.2810
Histopathological evaluation of recurrent hepatitis C after liver transplantation: a review
Abstract
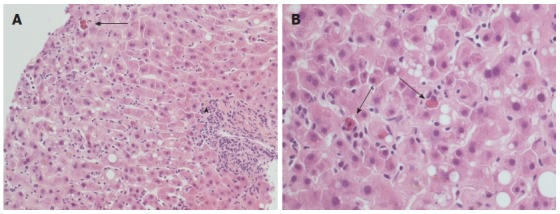
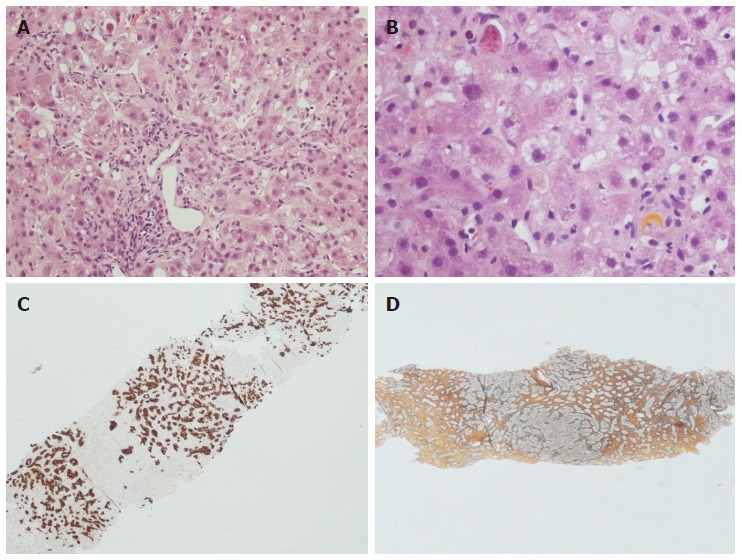
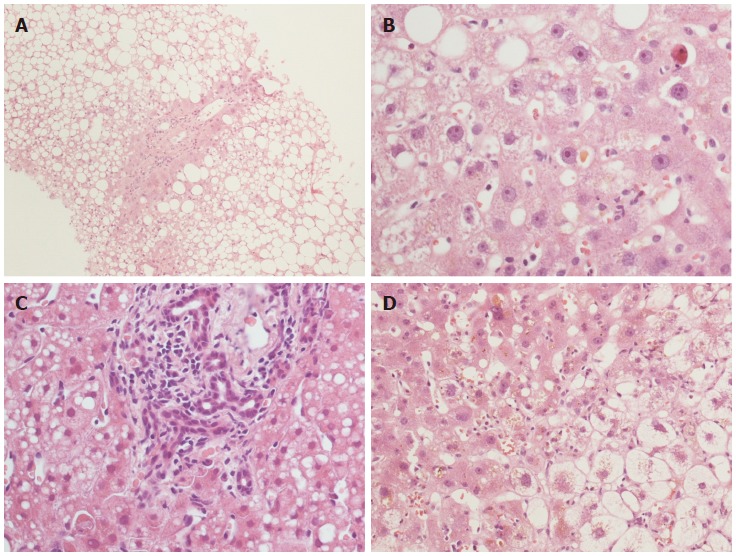
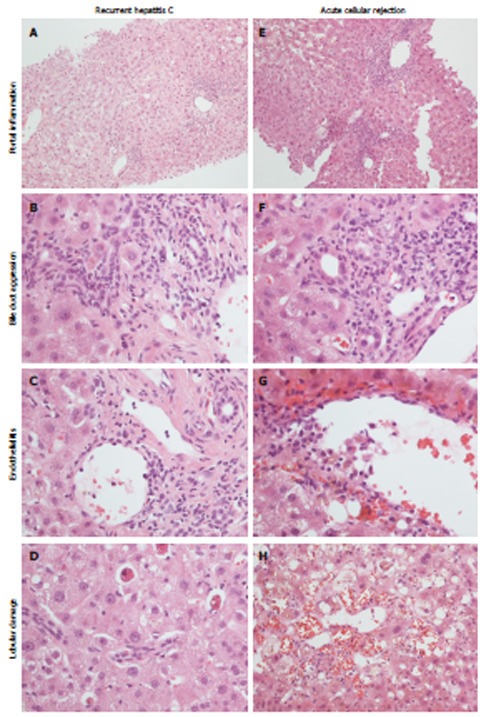
Although the morphological features of hepatitis C virus (HCV) recurrence after orthotopic liver transplantation (OLT) have been well established in the last decades, the differential diagnosis still represents a challenge for the pathologist, especially early recurrent hepatitis C vs mild acute cellular rejection. The present review focuses on the role of the pathologist and the pathology laboratory in the management of recipients with recurrent hepatitis C, the usefulness of early and late post-OLT liver biopsies, and the potential role of ancillary techniques (immunohistochemistry and reverse transcription-polymerase chain reaction, RT-PCR). The English literature on the topic is reviewed, focusing on the histopathology, the immunohistochemistry and the use of RT-PCR on HCV-positive post-OLT biopsies. The different histopathological illustrations of early and chronic recurrent hepatitis C are presented, with special focus on the main differential diagnoses and those features with prognostic relevance (cholestasis above all). The usefulness of ancillary techniques are discussed, especially HCV RNA quantitation by RT-PCR. Finally, the usefulness of long-term protocol biopsies is addressed: their usefulness for the study of allograft disease progression is clear, but their meaning in the long term is still debated. The significance of plasma cell infiltrate in HCV-positive allografts, the prognostic weight of graft steatosis, and the impact of donor age in recurrent hepatitis C also represent additional open issues.
Keywords: Hepatitis C virus; Histopathology; Immunohistochemistry; Orthotopic liver transplantation; Polymerase chain reaction; Recurrent hepatitis C.
Figures
References
-
- Terrault N. Liver transplantation in the setting of chronic HCV. Best Pract Res Clin Gastroenterol. 2012;26:531–548. - PubMed
-
- Belli LS, Alberti A, Rondinara GF, de Carlis L, Romani F, Ideo G, Belli L. Recurrent HCV hepatitis after liver transplantation. Lancet. 1993;341:378. - PubMed
-
- Shiffman ML, Contos MJ, Luketic VA, Sanyal AJ, Purdum PP, Mills AS, Fisher RA, Posner MP. Biochemical and histologic evaluation of recurrent hepatitis C following orthotopic liver transplantation. Transplantation. 1994;57:526–532. - PubMed
-
- Greenson JK, Svoboda-Newman SM, Merion RM, Frank TS. Histologic progression of recurrent hepatitis C in liver transplant allografts. Am J Surg Pathol. 1996;20:731–738. - PubMed
-
- Gane EJ, Portmann BC, Naoumov NV, Smith HM, Underhill JA, Donaldson PT, Maertens G, Williams R. Long-term outcome of hepatitis C infection after liver transplantation. N Engl J Med. 1996;334:815–820. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
