

Prediction of gait recovery in spinal cord injured individuals trained with robotic gait orthosis
- PMID: 24661681
- PMCID: PMC3987889
- DOI: 10.1186/1743-0003-11-42
Prediction of gait recovery in spinal cord injured individuals trained with robotic gait orthosis
Abstract
Background: Motor impairment is a major consequence of spinal cord injury (SCI). Earlier studies have shown that robotic gait orthosis (e.g., Lokomat) can improve an SCI individual's walking capacity. However, little is known about the differential responses among different individuals with SCI. The present longitudinal study sought to characterize the distinct recovery patterns of gait impairment for SCI subjects receiving Lokomat training, and to identify significant predictors for these patterns.
Methods: Forty SCI subjects with spastic hypertonia at their ankles were randomly allocated to either control or intervention groups. Subjects in the intervention group participated in twelve 1-hour Lokomat trainings over one month, while control subjects received no interventions. Walking capacity was evaluated in terms of walking speed, functional mobility, and endurance four times, i.e. baseline, 1, 2, and 4 weeks after training, using the 10-Meter-Walking, Timed-Up-and-Go, and 6-Minute-Walking tests. Growth Mixture Modeling, an analytical framework for stratifying subjects based on longitudinal changes, was used to classify subjects, based on their gait impairment recovery patterns, and to identify the effects of Lokomat training on these improvements.
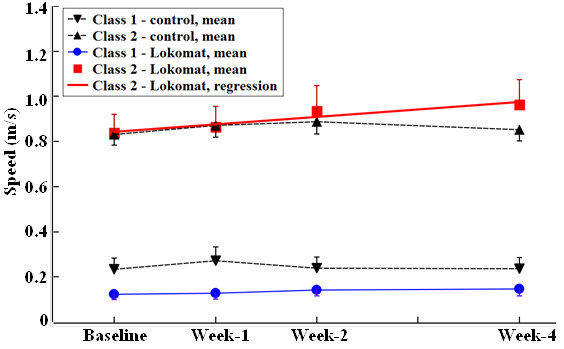
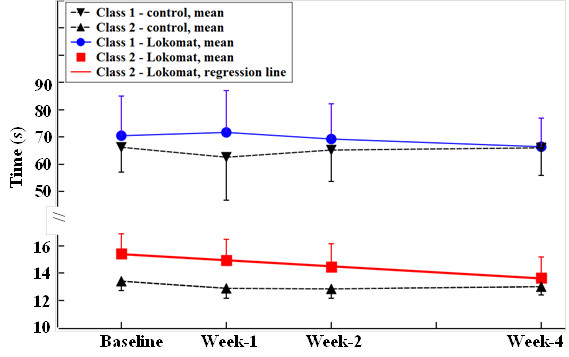
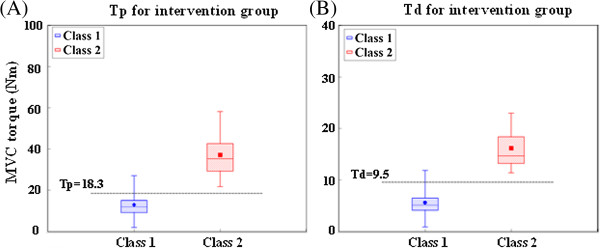
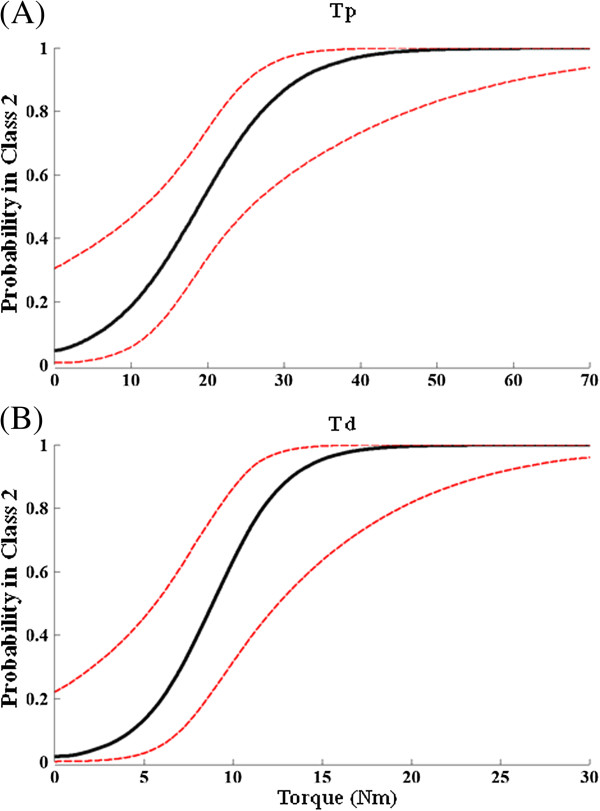
Results: Two recovery classes (low and high walking capacity) were identified for each clinical evaluation from both the control and intervention groups. Subjects with initial high walking capacity (i.e. shorter Timed-Up-and-Go time, higher 10-Meter-Walking speed and longer 6-Minute-Walking distance) displayed significant improvements in speed and functional mobility (0.033 m/s/week and-0.41 s/week respectively); however no significant change in endurance was observed. Subjects with low walking capacity exhibited no significant improvement. The membership in these two classes-and thus prediction of the subject's gait improvement trajectory over time-could be determined by the subject's maximum voluntary torque at the ankle under both plantar-and dorsi-flexion contractions determined prior to any training.
Conclusion: Our findings demonstrate that subjects responded to Lokomat training non-uniformly, and should potentially be grouped based on their likely recovery patterns using objective criteria. Further, we found that the subject's ankle torque can predict whether he/she would benefit most from Lokomat training prior to the therapy. These findings are clinically significant as they can help individualize therapeutic programs that maximize patient recovery while minimizing unnecessary efforts and costs.
Figures
Similar articles
-
Ankle voluntary movement enhancement following robotic-assisted locomotor training in spinal cord injury.J Neuroeng Rehabil. 2014 Mar 31;11:46. doi: 10.1186/1743-0003-11-46. J Neuroeng Rehabil. 2014. PMID: 24684813 Free PMC article. Clinical Trial.
-
The effect of impedance-controlled robotic gait training on walking ability and quality in individuals with chronic incomplete spinal cord injury: an explorative study.J Neuroeng Rehabil. 2014 Mar 4;11:26. doi: 10.1186/1743-0003-11-26. J Neuroeng Rehabil. 2014. PMID: 24594284 Free PMC article. Clinical Trial.
-
Prospective, blinded, randomized crossover study of gait rehabilitation in stroke patients using the Lokomat gait orthosis.Neurorehabil Neural Repair. 2007 Jul-Aug;21(4):307-14. doi: 10.1177/1545968307300697. Epub 2007 May 2. Neurorehabil Neural Repair. 2007. PMID: 17476001 Clinical Trial.
-
Comparative efficacy of robotic exoskeleton and conventional gait training in patients with spinal cord injury: a meta-analysis of randomized controlled trials.J Neuroeng Rehabil. 2025 May 29;22(1):121. doi: 10.1186/s12984-025-01649-1. J Neuroeng Rehabil. 2025. PMID: 40442684 Free PMC article.
-
Robotic rehabilitation of spinal cord injury individual.Ortop Traumatol Rehabil. 2013 Jan-Feb;15(1):1-7. doi: 10.5604/15093492.1032792. Ortop Traumatol Rehabil. 2013. PMID: 23510817 Review.
Cited by
-
Effects of body weight support and guidance force settings on muscle synergy during Lokomat walking.Eur J Appl Physiol. 2021 Nov;121(11):2967-2980. doi: 10.1007/s00421-021-04762-w. Epub 2021 Jul 4. Eur J Appl Physiol. 2021. PMID: 34218291
-
Effect of EMG-biofeedback robotic-assisted body weight supported treadmill training on walking ability and cardiopulmonary function on people with subacute spinal cord injuries - a randomized controlled trial.BMC Neurol. 2019 Jun 24;19(1):140. doi: 10.1186/s12883-019-1361-z. BMC Neurol. 2019. PMID: 31234791 Free PMC article. Clinical Trial.
-
Effects of robotic-locomotor training on stretch reflex function and muscular properties in individuals with spinal cord injury.Clin Neurophysiol. 2015 May;126(5):997-1006. doi: 10.1016/j.clinph.2014.09.010. Epub 2014 Sep 22. Clin Neurophysiol. 2015. PMID: 25449559 Free PMC article.
-
The Effectiveness and Safety of Exoskeletons as Assistive and Rehabilitation Devices in the Treatment of Neurologic Gait Disorders in Patients with Spinal Cord Injury: A Systematic Review.Global Spine J. 2016 Dec;6(8):822-841. doi: 10.1055/s-0036-1593805. Epub 2016 Nov 3. Global Spine J. 2016. PMID: 27853668 Free PMC article.
-
The effects of robot assisted gait training on temporal-spatial characteristics of people with spinal cord injuries: A systematic review.J Spinal Cord Med. 2018 Sep;41(5):529-543. doi: 10.1080/10790268.2018.1426236. Epub 2018 Feb 5. J Spinal Cord Med. 2018. PMID: 29400988 Free PMC article.
References
-
- Behrman AL, Harkema SJ. Locomotor training after human spinal cord injury: a series of case studies. Phys Ther. 2000;80:688–700. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
