

A systematic review of the effects of resident duty hour restrictions in surgery: impact on resident wellness, training, and patient outcomes
- PMID: 24662409
- PMCID: PMC4047317
- DOI: 10.1097/SLA.0000000000000595
A systematic review of the effects of resident duty hour restrictions in surgery: impact on resident wellness, training, and patient outcomes
Abstract
Background: In 2003, the Accreditation Council for Graduate Medical Education (ACGME) mandated 80-hour resident duty limits. In 2011 the ACGME mandated 16-hour duty maximums for PGY1 (post graduate year) residents. The stated goals were to improve patient safety, resident well-being, and education. A systematic review and meta-analysis were performed to evaluate the impact of resident duty hours (RDH) on clinical and educational outcomes in surgery.
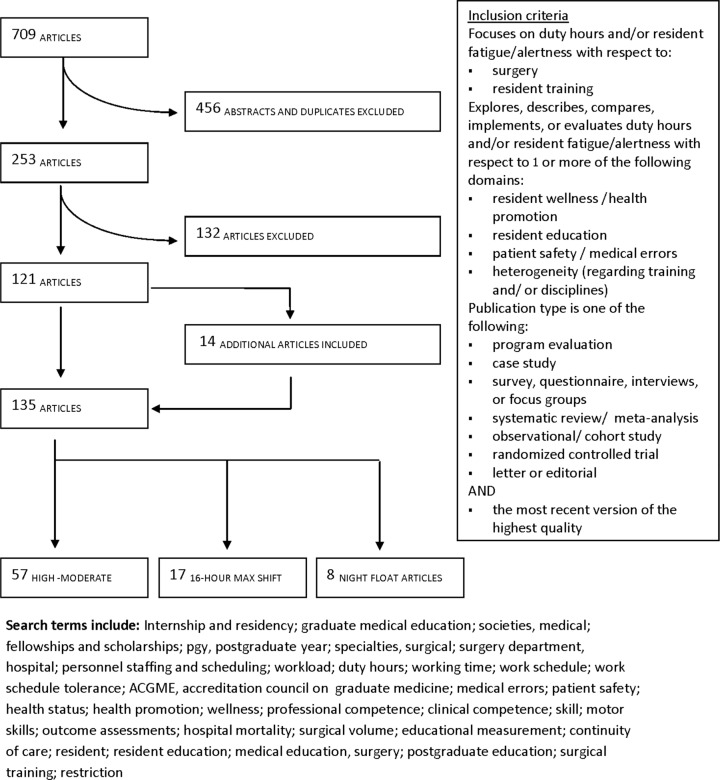
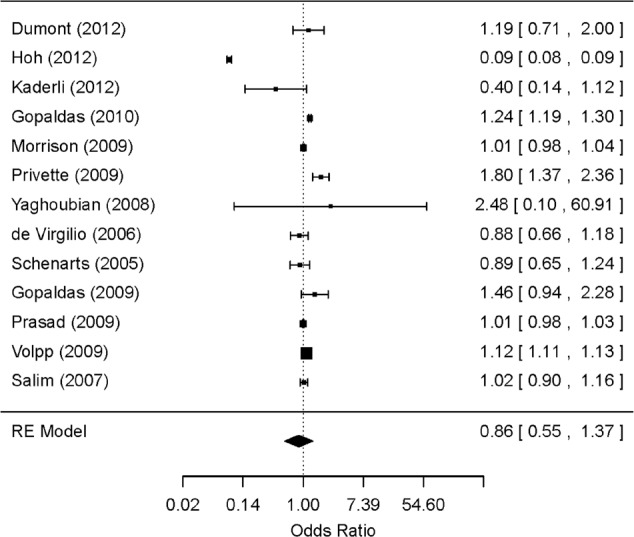
Methods: A systematic review (1980-2013) was executed on CINAHL, Cochrane Database, Embase, Medline, and Scopus. Quality of articles was assessed using the GRADE guidelines. Sixteen-hour shifts and night float systems were analyzed separately. Articles that examined mortality data were combined in a random-effects meta-analysis to evaluate the impact of RDH on patient mortality.
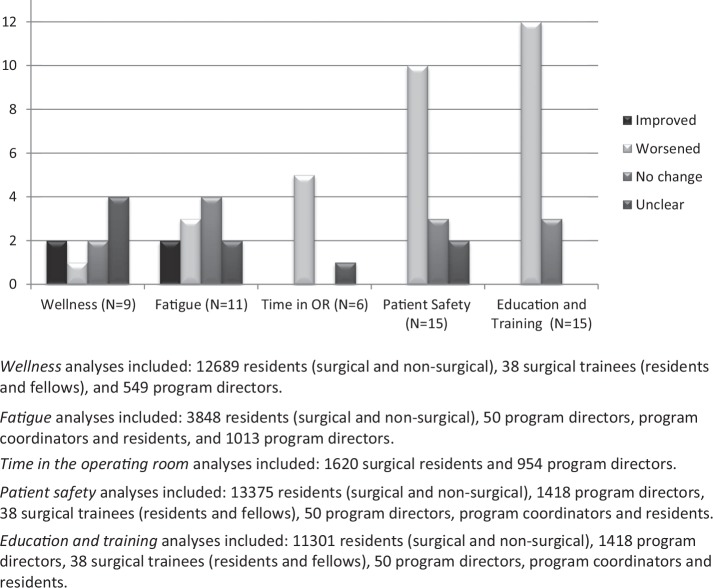
Results: A total of 135 articles met the inclusion criteria. Among these, 42% (N = 57) were considered moderate-high quality. There was no overall improvement in patient outcomes as a result of RDH; however, some studies suggest increased complication rates in high-acuity patients. There was no improvement in education related to RDH restrictions, and performance on certification examinations has declined in some specialties. Survey studies revealed a perception of worsened education and patient safety. There were improvements in resident wellness after the 80-hour workweek, but there was little improvement or negative effects on wellness after 16-hour duty maximums were implemented.
Conclusions: Recent RDH changes are not consistently associated with improvements in resident well-being, and have negative impacts on patient outcomes and performance on certification examinations. Greater flexibility to accommodate resident training needs is required. Further erosion of training time should be considered with great caution.
Figures
Comment in
-
Reduced surgical training hours harm patients and education, Canada study finds.BMJ. 2014 Apr 7;348:g2627. doi: 10.1136/bmj.g2627. BMJ. 2014. PMID: 24711669 No abstract available.
-
Commentary on "Resident work-hour restrictions and responsibilities to patients".Ann Surg. 2014 Jun;259(6):1054-5. doi: 10.1097/SLA.0000000000000700. Ann Surg. 2014. PMID: 24814502 No abstract available.
References
-
- Nasca TJ. An Open Letter to the GME Community. Chicago, IL: Accreditation Council for Graduate Medical Education; 2010
-
- Temple J. Time for Training: A Review of the impact of the European Working Time Directive on the Quality of Training. London, UK: Royal College of Surgeons of England; 2010
-
- American College of Surgeons Task Force. Position of the American College of Surgeons on restrictions on resident work hours. Paper presented at: The Institute of Medicine of the National Academies, Committee on Optimizing Graduate Medical Trainee (Resident) Schedules to Improve Patient Safety; March 4, 2008; Irvine, CA
-
- Drolet B, Sangisetty S, Tracy T, et al. Surgical residents' perceptions of 2011 Accreditation Council for Graduate Medical Education duty hour regulations. JAMA Surg. 2013;148:427–433 - PubMed
-
- National Steering Committee on Resident Duty Hours. Fatigue, Risk, & Excellence: Towards a Pan-Canadian Consensus on Resident Duty Hours. Ottawa, ON: Royal College of Physicians and Surgeons of Canada; 2013
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
