

Long-term financial burden of breast cancer: experiences of a diverse cohort of survivors identified through population-based registries
- PMID: 24663041
- PMCID: PMC3986387
- DOI: 10.1200/JCO.2013.53.0956
Long-term financial burden of breast cancer: experiences of a diverse cohort of survivors identified through population-based registries
Abstract
Purpose: To evaluate the financial experiences of a racially and ethnically diverse cohort of long-term breast cancer survivors (17% African American, 40% Latina) identified through population-based registries.
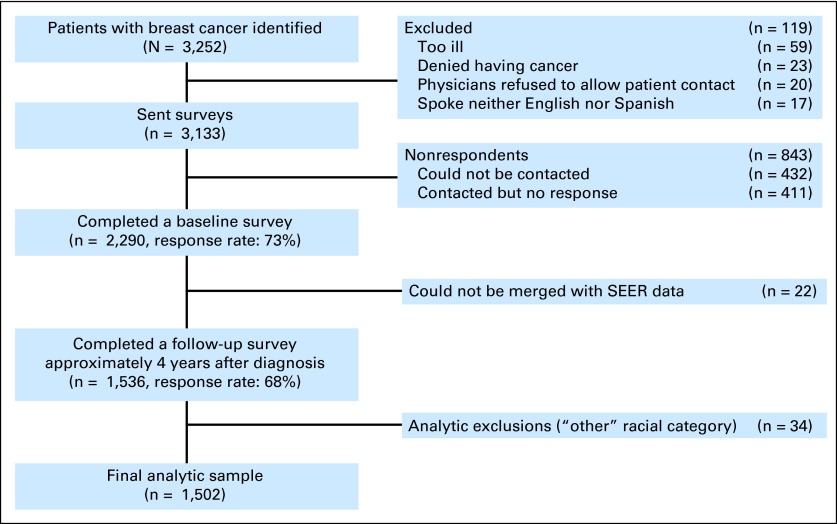
Methods: Longitudinal study of women diagnosed with nonmetastatic breast cancer in 2005 to 2007 and reported to the SEER registries of metropolitan Los Angeles and Detroit. We surveyed 3,133 women approximately 9 months after diagnosis and 4 years later. Multivariable models evaluated correlates of self-reported decline in financial status attributed to breast cancer and of experiencing at least one type of privation (economically motivated treatment nonadherence and broader hardships related to medical expenses).
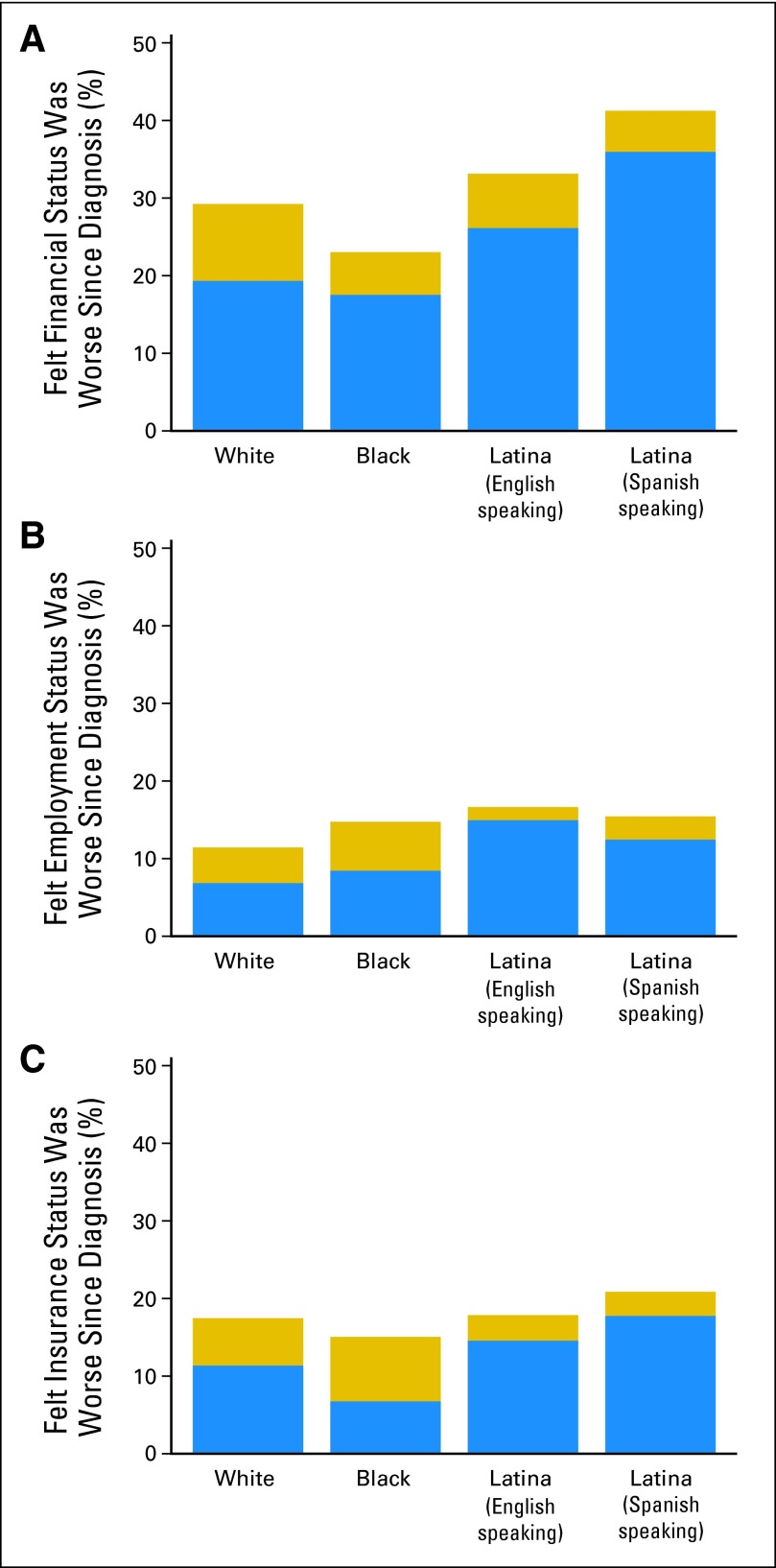
Results: Among 1,502 patients responding to both surveys, median out-of-pocket expenses were ≤ $2,000; 17% of respondents reported spending > $5,000; 12% reported having medical debt 4 years postdiagnosis. Debt varied significantly by race: 9% of whites, 15% of blacks, 17% of English-speaking Latinas, and 10% of Spanish-speaking Latinas reported debt (P = .03). Overall, 25% of women experienced financial decline at least partly attributed to breast cancer; Spanish-speaking Latinas had significantly increased odds of this decline relative to whites (odds ratio [OR], 2.76; P = .006). At least one privation was experienced by 18% of the sample; blacks (OR, 2.6; P < .001) and English-speaking Latinas (OR, 2.2; P = .02) were significantly more likely to have experienced privation than whites.
Conclusion: Racial and ethnic minority patients appear most vulnerable to privations and financial decline attributable to breast cancer, even after adjustment for income, education, and employment. These findings should motivate efforts to control costs and ensure communication between patients and providers regarding financial distress, particularly for vulnerable subgroups.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
References
-
- Bach PB, Saltz LB, Wittes RE. The New York Times; 2012. Oct 14, In cancer care, cost matters; p. A25. http://www.nytimes.com/2012/10/15/opinion/a-hospital-says-no-to-an-11000....
-
- Moriates C, Shah NT, Arora VM. First, do no (financial) harm. JAMA. 2013;310:577–578. - PubMed
-
- Kaiser Family Foundation and Health Research & Trust. Employer health benefits, 2013 annual survey. http://ehbs.kff.org/pdf/2011/8225.pdf.
-
- Howard DH, Molinari NA, Thorpe KE. National estimates of medical costs incurred by nonelderly cancer patients. Cancer. 2004;100:883–891. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
