

Stand up to cancer phase Ib study of pan-phosphoinositide-3-kinase inhibitor buparlisib with letrozole in estrogen receptor-positive/human epidermal growth factor receptor 2-negative metastatic breast cancer
- PMID: 24663045
- PMCID: PMC3986383
- DOI: 10.1200/JCO.2013.54.0518
Stand up to cancer phase Ib study of pan-phosphoinositide-3-kinase inhibitor buparlisib with letrozole in estrogen receptor-positive/human epidermal growth factor receptor 2-negative metastatic breast cancer
Abstract
Purpose: Buparlisib, an oral reversible inhibitor of all class I phosphoinositide-3-kinases, has shown antitumoral activity against estrogen receptor (ER)-positive breast cancer cell lines and xenografts, alone and with endocrine therapy. This phase Ib study evaluated buparlisib plus letrozole's safety, tolerability, and preliminary activity in patients with metastatic ER-positive breast cancer refractory to endocrine therapy.
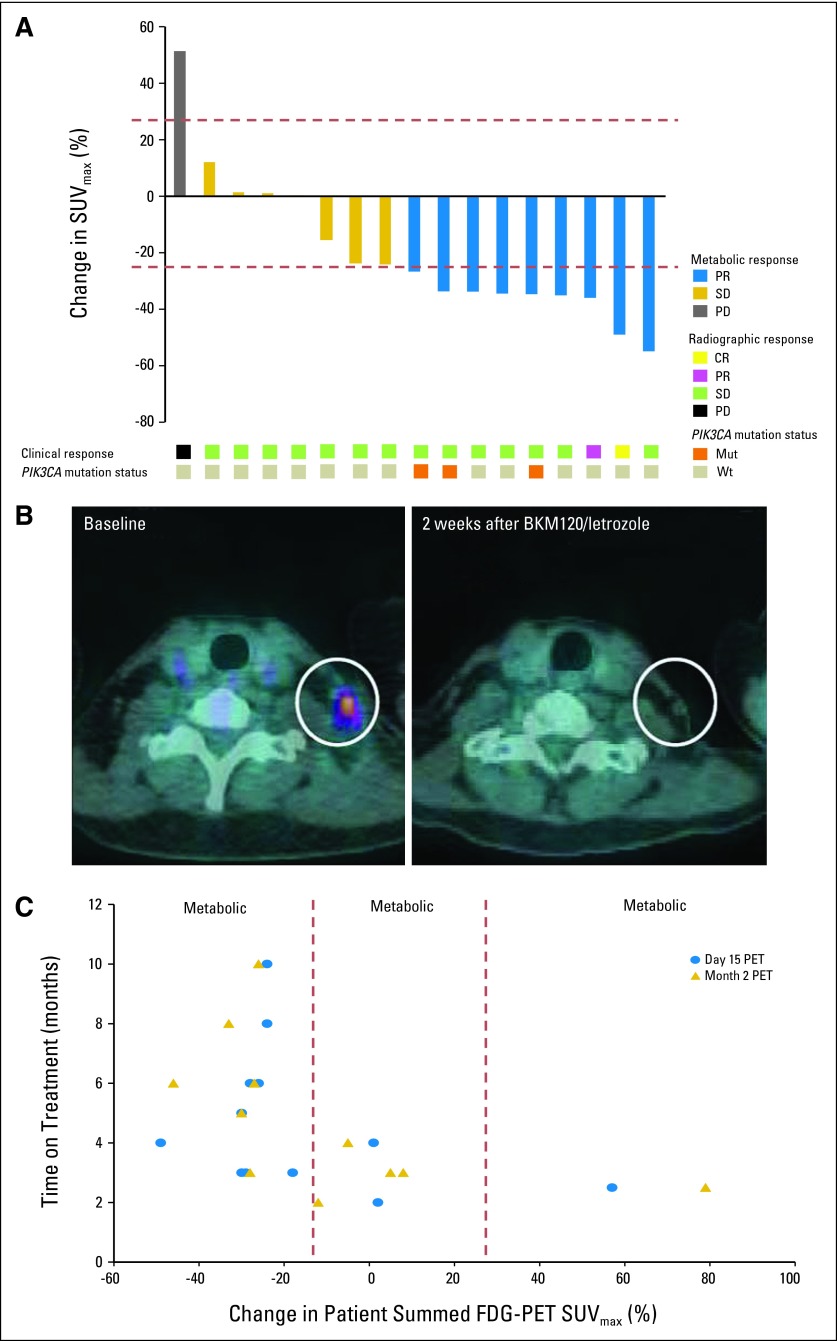
Patients and methods: Patients received letrozole and buparlisib in two different administration schedules. Outcomes were assessed by standard solid-tumor phase I methods. [(18)F]fluorodeoxyglucose-positron emission tomography/computed tomography ([(18)F]FDG-PET/CT) scans were done at baseline and 2 weeks after treatment initiation. Tumor blocks were collected for phosphoinositide-3-kinase pathway mutation analysis.
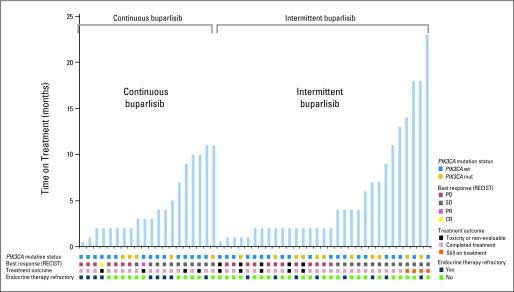
Results: Fifty-one patients were allocated sequentially to continuous or intermittent (five on/two off days) buparlisib administration on an every-4-week schedule. Buparlisib's maximum-tolerated dose (MTD) was 100 mg/d. Common drug-related adverse events included ≤ grade 2 hyperglycemia, nausea, fatigue, transaminitis, and mood disorders. The clinical benefit rate (lack of progression ≥ 6 months) among all patients treated at the MTD was 31%, including two objective responses in the continuous dose arm. Of seven patients remaining on treatment ≥ 12 months, three had tumors with PIK3CA hot-spot mutation. Patients exhibiting metabolic disease progression by [(18)F]FDG-PET/CT scan at 2 weeks progressed rapidly on therapy.
Conclusion: The letrozole and buparlisib combination was safe, with reversible toxicities regardless of schedule administration. Clinical activity was observed independent of PIK3CA mutation status. No metabolic response by [(18)F]FDG-PET/CT scan at 2 weeks was associated with rapid disease progression. Phase III trials of buparlisib and endocrine therapy in patients with ER-positive breast cancer are ongoing.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
References
-
- Samuels Y, Diaz LA, Jr, Schmidt-Kittler O, et al. Mutant PIK3CA promotes cell growth and invasion of human cancer cells. Cancer Cell. 2005;7:561–573. - PubMed
-
- Isakoff SJ, Engelman JA, Irie HY, et al. Breast cancer-associated PIK3CA mutations are oncogenic in mammary epithelial cells. Cancer Res. 2005;65:10992–11000. - PubMed
-
- Perez-Tenorio G, Alkhori L, Olsson B, et al. PIK3CA mutations and PTEN loss correlate with similar prognostic factors and are not mutually exclusive in breast cancer. Clin Cancer Res. 2007;13:3577–3584. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
