

Bedside tool for predicting the risk of postoperative atrial fibrillation after cardiac surgery: the POAF score
- PMID: 24663335
- PMCID: PMC4187480
- DOI: 10.1161/JAHA.113.000752
Bedside tool for predicting the risk of postoperative atrial fibrillation after cardiac surgery: the POAF score
Abstract
Background: Atrial fibrillation (AF) remains the most common complication after cardiac surgery. The present study aim was to derive an effective bedside tool to predict postoperative AF and its related complications.
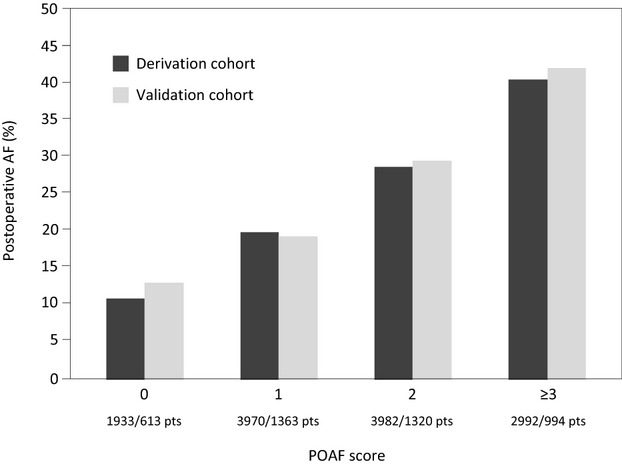
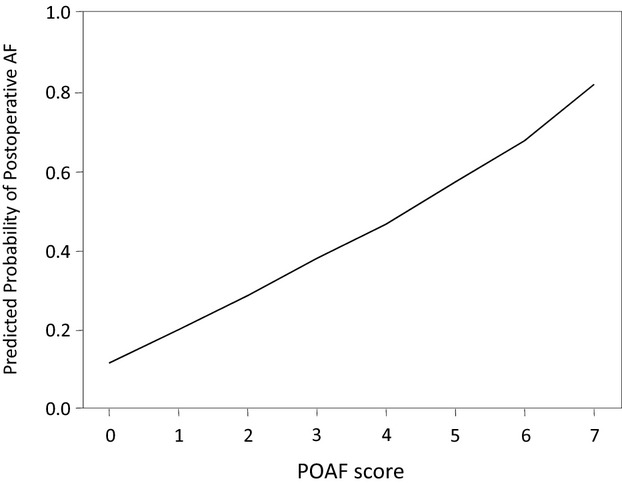
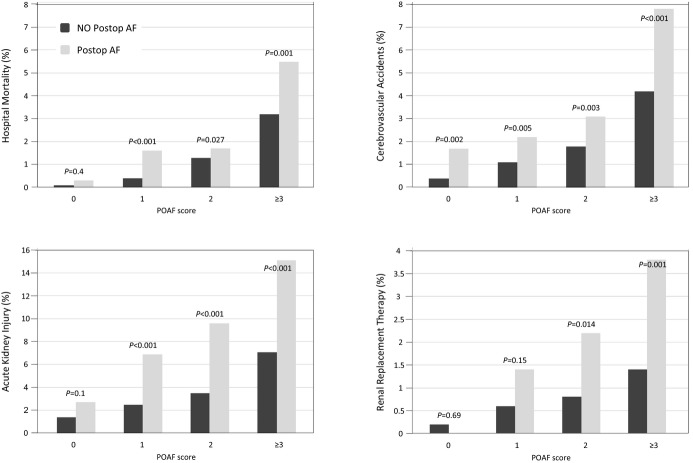
Methods and results: Data of 17 262 patients undergoing adult cardiac surgery were retrieved at 3 European university hospitals. A risk score for postoperative AF (POAF score) was derived and validated. In the overall series, 4561 patients (26.4%) developed postoperative AF. In the derivation cohort age, chronic obstructive pulmonary disease, emergency operation, preoperative intra-aortic balloon pump, left ventricular ejection fraction <30%, estimated glomerular filtration rate <15 mL/min per m(2) or dialysis, and any heart valve surgery were independent AF predictors. POAF score was calculated by summing weighting points for each independent AF predictor. According to the prediction model, the incidences of postoperative AF in the derivation cohort were 0, 11.1%; 1, 20.1%; 2, 28.7%; and ≥3, 40.9% (P<0.001), and in the validation cohort they were 0, 13.2%; 1, 19.5%; 2, 29.9%; and ≥3, 42.5% (P<0.001). Patients with a POAF score ≥3, compared with those without arrhythmia, revealed an increased risk of hospital mortality (5.5% versus 3.2%, P=0.001), death after the first postoperative day (5.1% versus 2.6%, P<0.001), cerebrovascular accident (7.8% versus 4.2%, P<0.001), acute kidney injury (15.1% versus 7.1%, P<0.001), renal replacement therapy (3.8% versus 1.4%, P<0.001), and length of hospital stay (mean 13.2 versus 10.2 days, P<0.001).
Conclusions: The POAF score is a simple, accurate bedside tool to predict postoperative AF and its related or accompanying complications.
Keywords: antiarrhythmic prevention; atrial fibrillation; cardiac surgery; risk stratification.
Figures
References
-
- Villareal RP, Hariharan R, Liu BC, Kar B, Lee VV, Elayda M, Lopez JA, Rasekh A, Wilson JM, Massumi A. Postoperative atrial fibrillation and mortality after coronary artery bypass surgery. J Am Coll Cardiol. 2004; 43:742-748 - PubMed
-
- Mariscalco G, Klersy C, Zanobini M, Banach M, Ferrarese S, Borsani P, Cantore C, Biglioli P, Sala A. Atrial fibrillation after isolated coronary surgery affects late survival. Circulation. 2008; 118:1612-1618 - PubMed
-
- Mahoney EM, Thompson TD, Veledar E, Williams J, Weintraub WS. Cost‐effectiveness of targeting patients undergoing cardiac surgery for therapy with intravenous amiodarone to prevent atrial fibrillation. J Am Coll Cardiol. 2002; 40:737-745 - PubMed
-
- Mariscalco G, Engström KG. Atrial fibrillation after cardiac surgery: risk factors and their temporal relationship in prophylactic drug strategy decision. Int J Cardiol. 2008; 129:354-362 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
