

Regional chemotherapy for unresectable intrahepatic cholangiocarcinoma: a potential role for dynamic magnetic resonance imaging as an imaging biomarker and a survival update from two prospective clinical trials
- PMID: 24664624
- PMCID: PMC4516216
- DOI: 10.1245/s10434-014-3649-y
Regional chemotherapy for unresectable intrahepatic cholangiocarcinoma: a potential role for dynamic magnetic resonance imaging as an imaging biomarker and a survival update from two prospective clinical trials
Abstract
Background: For patients with unresectable intrahepatic cholangiocarcinoma (ICC), treatment options are limited and survival is poor. This study summarizes the long-term outcome of two previously reported clinical trials using hepatic arterial infusion (HAI) with floxuridine and dexamethasone (with or without bevacizumab) in advanced ICC.
Methods: Prospectively collected clinicopathologic and survival data were retrospectively reviewed. Response was based on Response Evaluation Criteria in Solid Tumors (RECIST). Pre-HAI dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) images were reviewed, and tumor perfusion data correlated with outcome.
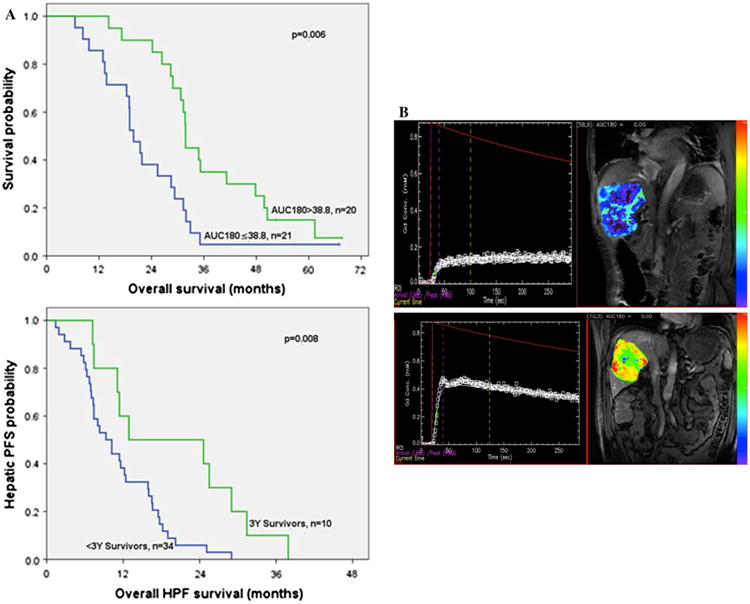
Results: Forty-four patients were analyzed (floxuridine, 26; floxuridine/bevacizumab, 18). At a median follow-up of 29.3 months, 41 patients had died of disease. Partial response by RECIST was observed in 48 %, and 50 % had stable disease. Three patients underwent resection after response, and 82 % received additional HAI after removal from the trials. Median survival was similar in both trials (floxuridine 29.3 months vs. floxuridine/bevacizumab 28.5 months; p = 0.96). Ten (23 %) patients survived ≥3 years, including 5 (11 %) who survived ≥5 years. Tumor perfusion measured on pre-treatment DCE-MRI [area under the gadolinium concentration curve at 90 and 180 s (AUC90 and AUC180, respectively)] was significantly higher in ≥3-year survivors and was the only factor that distinguished this group from <3-year survivors (mean AUC90 22.6 vs. 15.9 mM s, p = 0.025, and mean AUC180 48.9 vs. 32.3 mM s, p = 0.003, respectively). Median hepatic progression-free survival was longer in ≥3-year survivors (12.9 vs. 9.3 months, respectively; p = 0.008).
Conclusions: HAI chemotherapy can result in prolonged survival in unresectable ICC. Pre-HAI DCE-MRI may predict treatment outcome.
Figures
References
-
- Khan SA, Thomas HC, Davidson BR, Taylor-Robinson SD. Cholangiocarcinoma. Lancet. 2005;366(9493):1303–14. - PubMed
-
- Shaib Y, El-Serag HB. The epidemiology of cholangiocarcinoma. Semin Liver Dis. 2004;24(2):115–25. - PubMed
-
- Valle J, Wasan H, Palmer DH, Cunningham D, Anthoney A, Maraveyas A, et al. Cisplatin plus gemcitabine versus gemcitabine for biliary tract cancer. N Engl J Med. 2010;362(14):1273–81. - PubMed
-
- Sullivan RD, Norcross JW, Watkins E., Jr Chemotherapy of metastatic liver cancer by prolonged hepatic-artery infusion. N Engl J Med. 1964;270:321–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
