

High definition video teaching module for learning neck dissection
- PMID: 24666440
- PMCID: PMC3974416
- DOI: 10.1186/1916-0216-43-7
High definition video teaching module for learning neck dissection
Abstract
Introduction: Video teaching modules are proven effective tools for enhancing student competencies and technical skills in the operating room. Integration into post-graduate surgical curricula, however, continues to pose a challenge in modern surgical education. To date, video teaching modules for neck dissection have yet to be described in the literature.
Purpose: To develop and validate an HD video-based teaching module (HDVM) to help instruct post-graduate otolaryngology trainees in performing neck dissection.
Methods: This prospective study included 6 intermediate to senior otolaryngology residents. All consented subjects first performed a control selective neck dissection. Subjects were then exposed to the video teaching module. Following a washout period, a repeat procedure was performed. Recordings of the both sets of neck dissections were de-identified and reviewed by an independent evaluator and scored using the Observational Clinical Human Reliability Assessment (OCHRA) system.
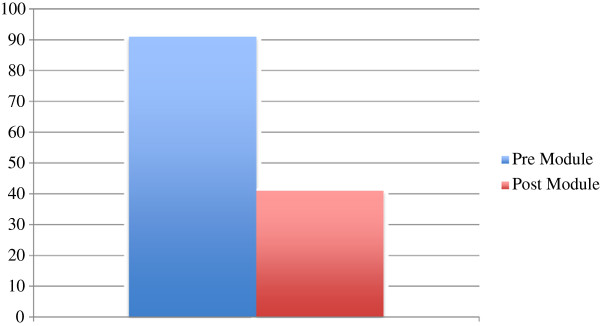
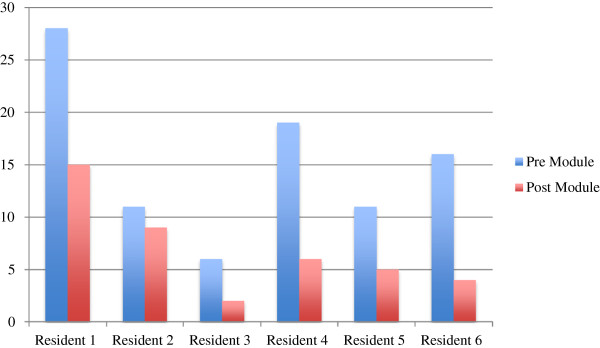
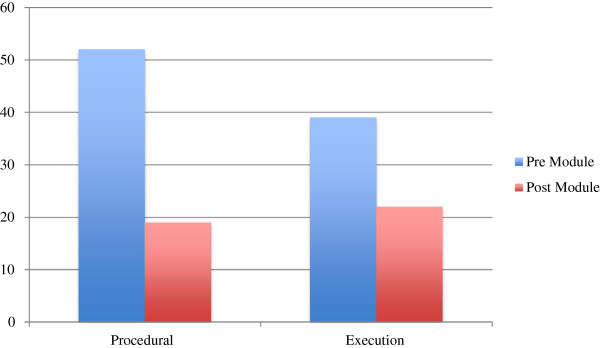
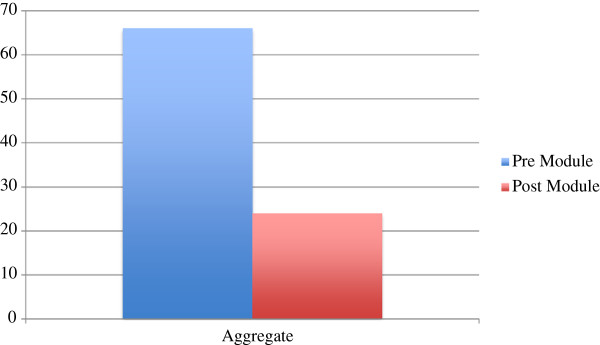
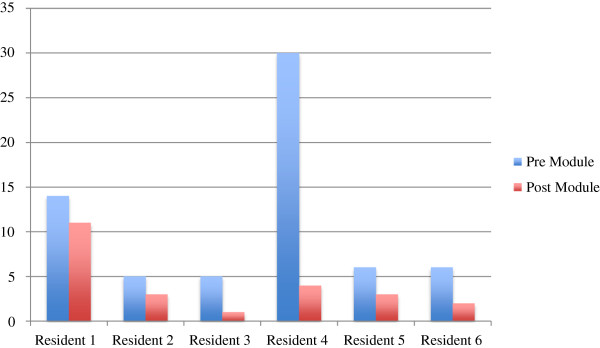
Results: In total 91 surgical errors were made prior to the HDVM and 41 after exposure, representing a 55% decrease in error occurrence. The two groups were found to be significantly different. Similarly, 66 and 24 staff takeover events occurred pre and post HDVM exposure, respectively, representing a statistically significant 64% decrease.
Conclusion: HDVM is a useful adjunct to classical surgical training. Residents performed significantly less errors following exposure to the HD-video module. Similarly, significantly less staff takeover events occurred following exposure to the HDVM.
Figures
References
-
- Palter VN, Grantcharov TP. Development and validation of a comprehensive curriculum to teach an advanced minimally invasive procedure: a randomized controlled trial. Ann Surg. 2012;256:25–32. - PubMed
-
- Tang B, Hanna GB, Cuschieri A. Analysis of errors enacted by surgical trainees during skills training courses. J. 2005;138:14–20. - PubMed
-
- Darzi A, Datta V, Mackay S. The challenge of objective assessment of surgical skill. Am J Surg. 2001;181:484–486. - PubMed
-
- Aggarwal R, Grantcharov TP, Darzi A. Framework for systematic training and assessment of technical skills. J Am Coll Surg. 2007;4:697–705. - PubMed
-
- Tang B, Hanna GB, Joice P, Cuschieri A. Identification and categorization of technical errors by observational clinical human reliability assessment (OCHRA) during laparoscopic cholecystectomy. Arch Surg. 2004;139:1215–1220. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
