

Neuro-intensive treatment targeting intracranial hypertension improves outcome in severe bacterial meningitis: an intervention-control study
- PMID: 24667767
- PMCID: PMC3965390
- DOI: 10.1371/journal.pone.0091976
Neuro-intensive treatment targeting intracranial hypertension improves outcome in severe bacterial meningitis: an intervention-control study
Abstract
Objective: To evaluate the efficacy of early intracranial pressure (ICP)-targeted treatment, compared to standard intensive care, in adults with community acquired acute bacterial meningitis (ABM) and severely impaired consciousness.
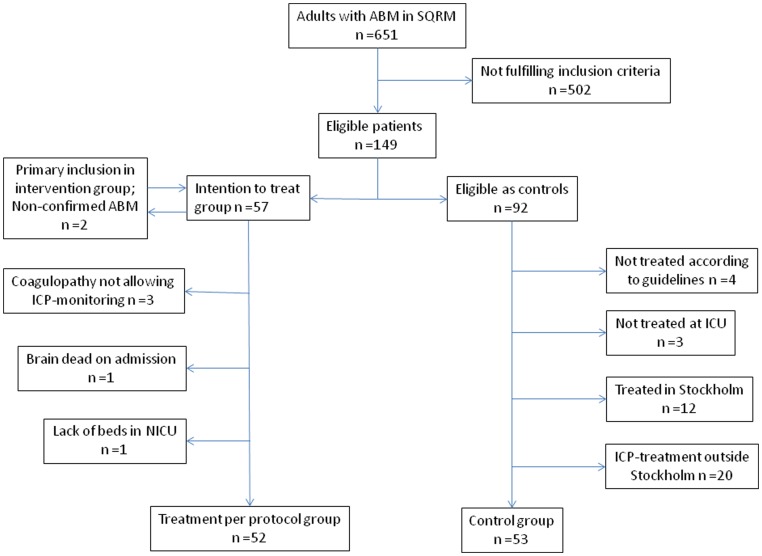
Design: A prospectively designed intervention-control comparison study of adult cases from September 2004 to January 2012.
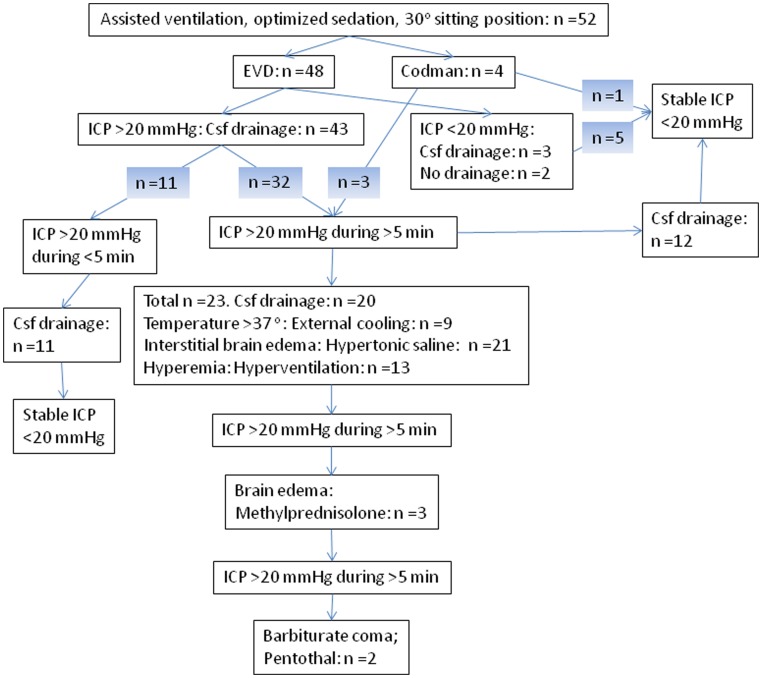
Patients: Included patients were confirmed ABM-cases, aged 16-75 years, with severely impaired mental status on admission. Fifty-two patients, given ICP-targeted treatment at the neuro-intensive care unit, and 53 control cases, treated with conventional intensive care, were included. All the patients received intensive care with mechanical ventilation, sedation, antibiotics and corticosteroids according to current guidelines. Additional ICP-treatment in the intervention group included cerebrospinal fluid drainage using external ventricular catheters (n = 48), osmotherapy (n = 21), hyperventilation (n = 13), external cooling (n = 9), gram-doses of methylprednisolone (n = 3) and deep barbiturate sedation (n = 2) aiming at ICP <20 mmHg and a cerebral perfusion pressure of >50 mmHg.
Measurements: The primary endpoint was mortality at two months and secondary endpoint was Glasgow outcome score and hearing ability at follow-up at 2-6 months.
Outcomes: The mortality was significantly lower in the intervention group compared to controls, 5/52 (10%) versus 16/53 (30%; relative risk reduction 68%; p<0.05). Furthermore, only 17 patients (32%) in the control group fully recovered compared to 28 (54%) in the intervention group (relative risk reduction 40%; p<0.05).
Conclusions: Early neuro-intensive care using ICP-targeted therapy, mainly cerebrospinal fluid drainage, reduces mortality and improves the overall outcome in adult patients with ABM and severely impaired mental status on admission.
Conflict of interest statement
Figures
Similar articles
-
[Intracranial pressure targeted treatment in acute bacterial meningitis increased survival].Lakartidningen. 2014 Dec 16;111(51-52):2288-91. Lakartidningen. 2014. PMID: 25514667 Clinical Trial. Swedish.
-
Lumbar drainage for the treatment of severe bacterial meningitis.Neurocrit Care. 2013 Oct;19(2):199-205. doi: 10.1007/s12028-013-9853-y. Neurocrit Care. 2013. PMID: 23739926
-
Randomized controlled trial comparing cerebral perfusion pressure-targeted therapy versus intracranial pressure-targeted therapy for raised intracranial pressure due to acute CNS infections in children.Crit Care Med. 2014 Aug;42(8):1775-87. doi: 10.1097/CCM.0000000000000298. Crit Care Med. 2014. PMID: 24690571 Clinical Trial.
-
Prevention and treatment of intracranial hypertension.Best Pract Res Clin Anaesthesiol. 2007 Dec;21(4):517-38. doi: 10.1016/j.bpa.2007.09.001. Best Pract Res Clin Anaesthesiol. 2007. PMID: 18286835 Review.
-
An overview of management of intracranial hypertension in the intensive care unit.J Anesth. 2020 Oct;34(5):741-757. doi: 10.1007/s00540-020-02795-7. Epub 2020 May 21. J Anesth. 2020. PMID: 32440802 Free PMC article. Review.
Cited by
-
Understanding coma in bacterial meningitis.Intensive Care Med. 2016 Aug;42(8):1282-5. doi: 10.1007/s00134-015-4074-9. Epub 2015 Sep 28. Intensive Care Med. 2016. PMID: 26415681 No abstract available.
-
What's new in bacterial meningitis.Intensive Care Med. 2016 Mar;42(3):415-417. doi: 10.1007/s00134-015-4057-x. Epub 2015 Sep 30. Intensive Care Med. 2016. PMID: 26424682 Free PMC article. Review. No abstract available.
-
A retrospective analysis of 20,178 adult neurological infection admissions to United Kingdom critical care units from 2001 to 2020.BMC Infect Dis. 2024 Jan 25;24(1):132. doi: 10.1186/s12879-024-08976-z. BMC Infect Dis. 2024. PMID: 38273223 Free PMC article.
-
[Acute care of patients with bacterial meningitis].Med Klin Intensivmed Notfmed. 2016 Apr;111(3):215-23. doi: 10.1007/s00063-015-0021-3. Epub 2015 Apr 16. Med Klin Intensivmed Notfmed. 2016. PMID: 25876743 Review. German.
-
Critical care management of infectious meningitis and encephalitis.Intensive Care Med. 2020 Feb;46(2):192-201. doi: 10.1007/s00134-019-05901-w. Epub 2020 Jan 14. Intensive Care Med. 2020. PMID: 31938828 No abstract available.
References
-
- de Gans J, van de Beek D, European Dexamethasone in Adulthood Bacterial Meningitis Study I (2002) Dexamethasone in adults with bacterial meningitis. The New England journal of medicine 347: 1549–1556. - PubMed
-
- Durand ML, Calderwood SB, Weber DJ, Miller SI, Southwick FS, et al. (1993) Acute bacterial meningitis in adults. A review of 493 episodes. N Engl J Med 328: 21–28. - PubMed
-
- Thigpen MC, Whitney CG, Messonnier NE, Zell ER, Lynfield R, et al. (2011) Bacterial meningitis in the United States, 1998–2007. N Engl J Med 364: 2016–2025. - PubMed
-
- van de Beek D (2012) Progress and challenges in bacterial meningitis. Lancet 380: 1623–1624. - PubMed
-
- van de Beek D, de Gans J, Spanjaard L, Weisfelt M, Reitsma JB, et al. (2004) Clinical features and prognostic factors in adults with bacterial meningitis. N Engl J Med 351: 1849–1859. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
