

Timing of tracheostomy in critically ill patients: a meta-analysis
- PMID: 24667875
- PMCID: PMC3965497
- DOI: 10.1371/journal.pone.0092981
Timing of tracheostomy in critically ill patients: a meta-analysis
Abstract
Objective: To compare important outcomes between early tracheostomy (ET) and late tracheostomy (LT) or prolonged intubation (PI) for critically ill patients receiving long-term ventilation during their treatment.
Method: We performed computerized searches for relevant articles on PubMed, EMBASE, and the Cochrane register of controlled trials (up to July 2013). We contacted international experts and manufacturers. We included in the study randomized controlled trials (RCTs) that compared ET (performed within 10 days after initiation of laryngeal intubation) and LT (after 10 days of laryngeal intubation) or PI in critically ill adult patients admitted to intensive care units (ICUs). Two investigators evaluated the articles; divergent opinions were resolved by consensus.
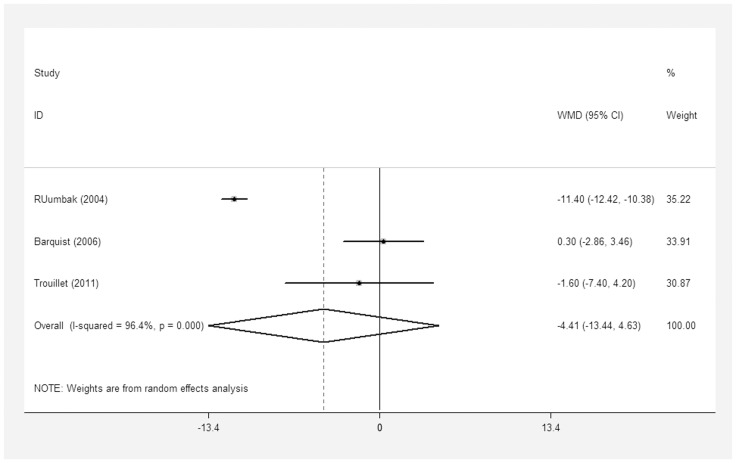
Results: A meta-analysis was evaluated from nine randomized clinical trials with 2,072 participants. Compared to LT/PI, ET did not significantly reduce short-term mortality [relative risks (RR) = 0.91; 95% confidence intervals (CIs) = 0.81-1.03; p = 0.14] or long-term mortality (RR = 0.90; 95% CI = 0.76-1.08; p = 0.27). Additionally, ET was not associated with a markedly reduced length of ICU stay [weighted mean difference (WMD) = -4.41 days; 95% CI = -13.44-4.63 days; p = 0.34], ventilator-associated pneumonia (VAP) (RR = 0.88; 95% CI = 0.71-1.10; p = 0.27) or duration of mechanical ventilation (MV) (WMD = - 2.91 days; 95% CI = -7.21-1.40 days; p = 0.19).
Conclusion: Among the patients requiring prolonged MV, ET showed no significant difference in clinical outcomes compared to that of the LT/PI group. But more rigorously designed and adequately powered RCTs are required to confirm it in future.
Conflict of interest statement
Figures







References
-
- Terra RM, Fernandez A, Bammann RH, Castro AC, Ishy A, et al. (2007) Open bedside tracheostomy: routine procedure for patients under prolonged mechanical ventilation. Clinics (Sao Paulo) 62 427–432: doi.org/10.1590/S1807–59322007000400009. - PubMed
-
- MacIntyre NR, Cook DJ, Ely EW Jr, Epstein SK, Fink JB, et al. (2001) Evidence-based guidelines for weaning and discontinuing ventilatory support: a collective task force facilitated by the American College of Chest Physicians; the American Association for Respiratory Care; and the American College of Critical Care Medicine. Chest 120: 375S–395S 10.1378/chest.120.6suppl.375S - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
