

Glycated hemoglobin measurement and prediction of cardiovascular disease
- PMID: 24668104
- PMCID: PMC4386007
- DOI: 10.1001/jama.2014.1873
Glycated hemoglobin measurement and prediction of cardiovascular disease
Abstract
Importance: The value of measuring levels of glycated hemoglobin (HbA1c) for the prediction of first cardiovascular events is uncertain.
Objective: To determine whether adding information on HbA1c values to conventional cardiovascular risk factors is associated with improvement in prediction of cardiovascular disease (CVD) risk.
Design, setting, and participants: Analysis of individual-participant data available from 73 prospective studies involving 294,998 participants without a known history of diabetes mellitus or CVD at the baseline assessment.
Main outcomes and measures: Measures of risk discrimination for CVD outcomes (eg, C-index) and reclassification (eg, net reclassification improvement) of participants across predicted 10-year risk categories of low (<5%), intermediate (5% to <7.5%), and high (≥ 7.5%) risk.
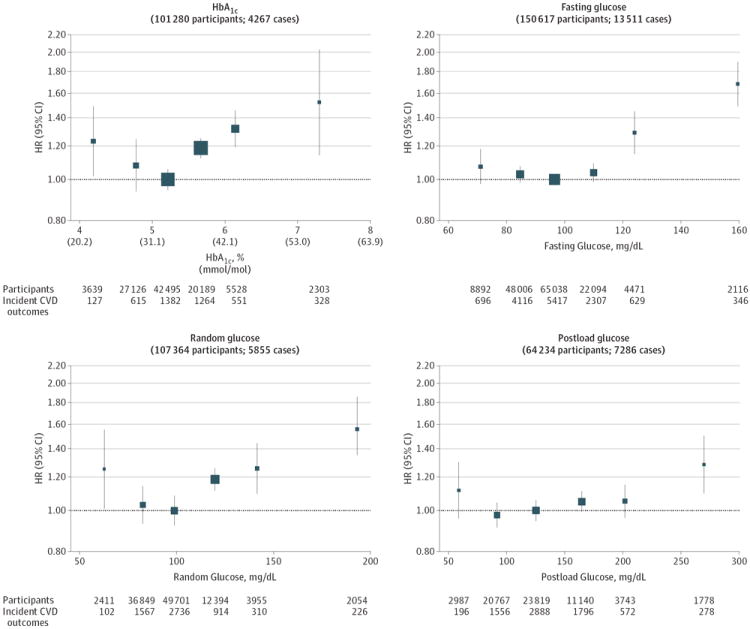
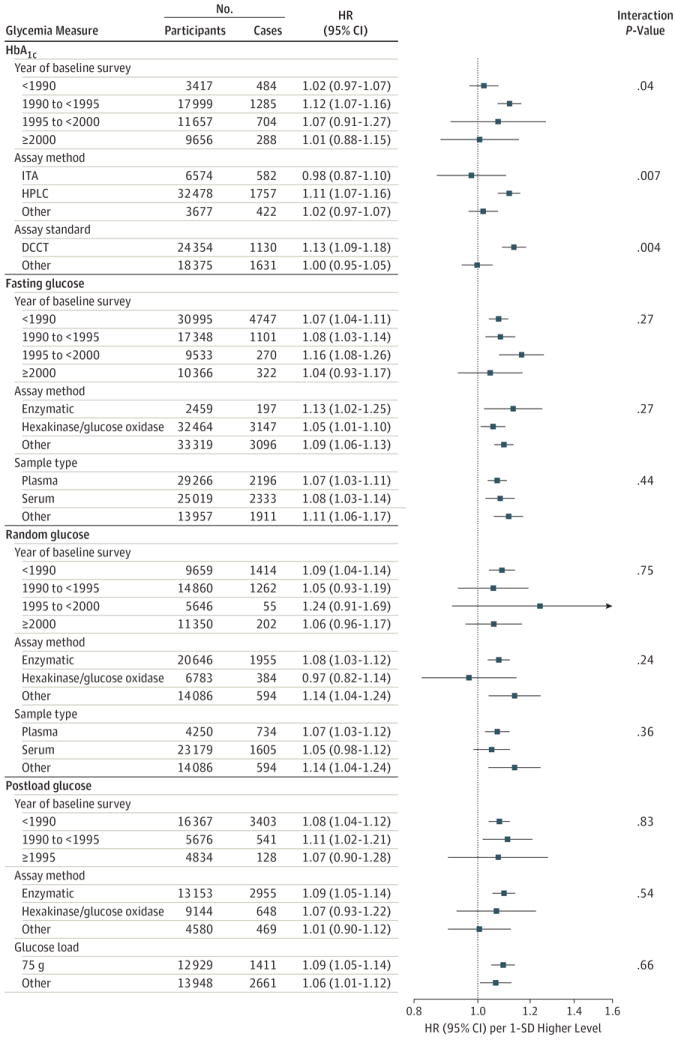
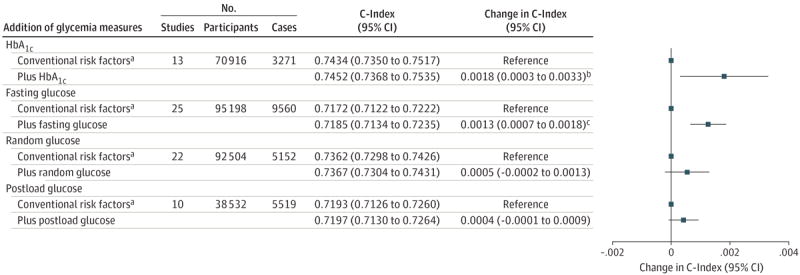
Results: During a median follow-up of 9.9 (interquartile range, 7.6-13.2) years, 20,840 incident fatal and nonfatal CVD outcomes (13,237 coronary heart disease and 7603 stroke outcomes) were recorded. In analyses adjusted for several conventional cardiovascular risk factors, there was an approximately J-shaped association between HbA1c values and CVD risk. The association between HbA1c values and CVD risk changed only slightly after adjustment for total cholesterol and triglyceride concentrations or estimated glomerular filtration rate, but this association attenuated somewhat after adjustment for concentrations of high-density lipoprotein cholesterol and C-reactive protein. The C-index for a CVD risk prediction model containing conventional cardiovascular risk factors alone was 0.7434 (95% CI, 0.7350 to 0.7517). The addition of information on HbA1c was associated with a C-index change of 0.0018 (0.0003 to 0.0033) and a net reclassification improvement of 0.42 (-0.63 to 1.48) for the categories of predicted 10-year CVD risk. The improvement provided by HbA1c assessment in prediction of CVD risk was equal to or better than estimated improvements for measurement of fasting, random, or postload plasma glucose levels.
Conclusions and relevance: In a study of individuals without known CVD or diabetes, additional assessment of HbA1c values in the context of CVD risk assessment provided little incremental benefit for prediction of CVD risk.
Figures
References
-
- Rydén L, Grant PJ, Anker SD, et al. Authors/Task Force Members; ESC Committee for Practice Guidelines (CPG); Document Reviewers. ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD: the Task Force on diabetes, pre-diabetes, and cardiovascular diseases of the European Society of Cardiology (ESC) and developed in collaboration with the European Association for the Study of Diabetes (EASD) Eur Heart J. 2013;34(39):3035–3087. - PubMed
-
- Sarwar N, Gao P, Seshasai SR, et al. Emerging Risk Factors Collaboration. Diabetes mellitus, fasting blood glucose concentration, and risk of vascular disease: a collaborative meta-analysis of 102 prospective studies. Lancet. 2010;375(9733):2215–2222. published correction appears in Lancet. 2010;376(9745):958. - PMC - PubMed
-
- US Preventive Services Task Force. Using nontraditional risk factors in coronary heart disease risk assessment: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2009;151(7):474–482. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- MC_UU_12015/4/MRC_/Medical Research Council/United Kingdom
- PG/13/66/30442/BHF_/British Heart Foundation/United Kingdom
- RG/08/014/24067/BHF_/British Heart Foundation/United Kingdom
- MR/L003120/1/MRC_/Medical Research Council/United Kingdom
- UL1 TR000062/TR/NCATS NIH HHS/United States
- G0401527/MRC_/Medical Research Council/United Kingdom
- MC_U106179474/MRC_/Medical Research Council/United Kingdom
- MR/K013351/1/MRC_/Medical Research Council/United Kingdom
- RG/13/16/30528/BHF_/British Heart Foundation/United Kingdom
- MC_UU_12013/5/MRC_/Medical Research Council/United Kingdom
- G1000143/MRC_/Medical Research Council/United Kingdom
- RG/08/013/25942/BHF_/British Heart Foundation/United Kingdom
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
