

The cost-effectiveness of improved hepatitis C virus therapies in HIV/hepatitis C virus coinfected patients
- PMID: 24670522
- PMCID: PMC4045405
- DOI: 10.1097/QAD.0000000000000093
The cost-effectiveness of improved hepatitis C virus therapies in HIV/hepatitis C virus coinfected patients
Abstract
Objectives: To evaluate the effectiveness and cost-effectiveness of strategies to treat hepatitis C virus (HCV) in HIV/HCV coinfected patients in the United States.
Participants: Simulated cohort of HIV/HCV genotype 1 coinfected, noncirrhotic, HCV treatment-naive individuals enrolled in US HIV guideline-concordant care.
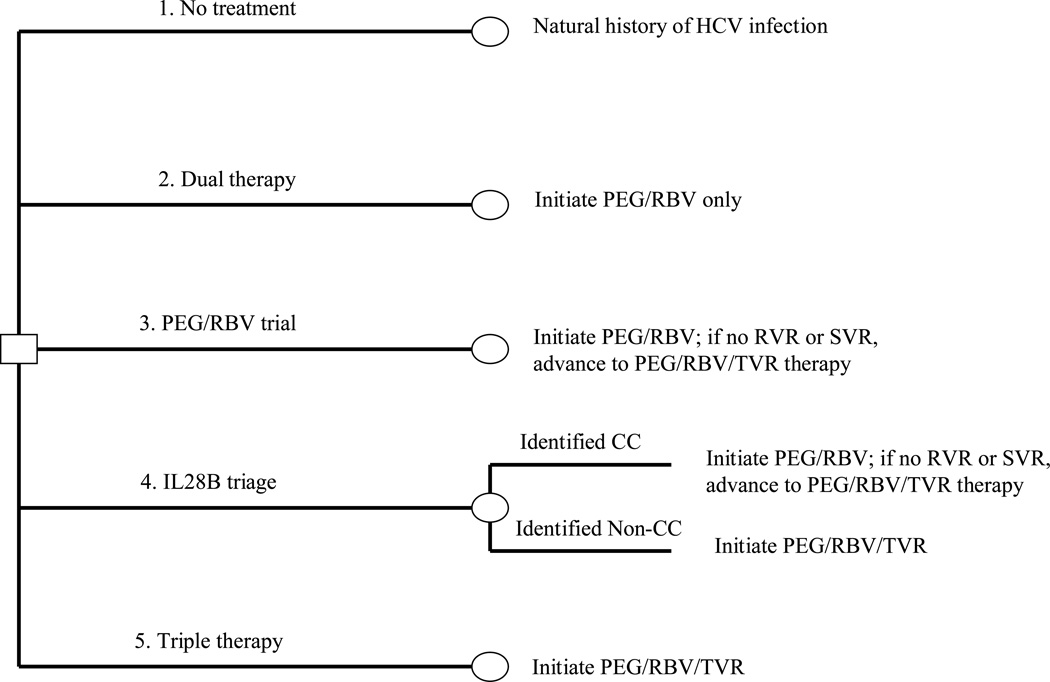
Design/interventions: Monte Carlo simulation comparing five strategies: no treatment; dual therapy with pegylated-interferon (PEG) and ribavirin (RBV); 'PEG/RBV trial' in which all patients initiate dual therapy and switch to triple therapy upon failure; 'IL28B triage' in which patients initiate either dual therapy or triple therapy based on their IL28B allele type; and PEG/RBV and telaprevir (TPV) triple therapy. Sensitivity analyses varied efficacies and costs and included a scenario with interferon (IFN)-free therapy.
Main measures: Sustained virologic response (SVR), life expectancy, discounted quality-adjusted life expectancy (QALE), lifetime medical costs, and incremental cost-effectiveness ratios (ICERs) in $/quality-adjusted life years (QALY) gained.
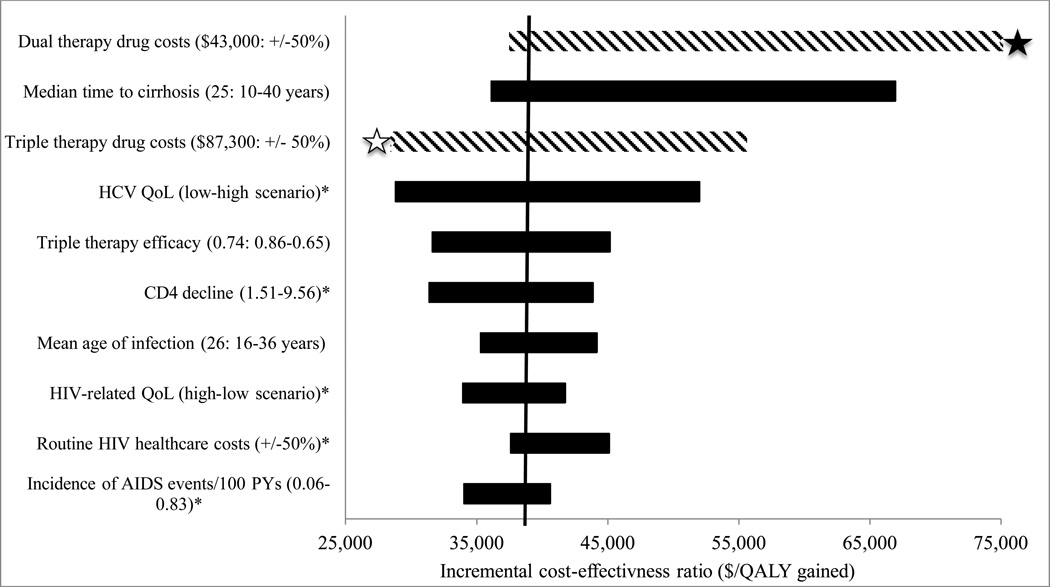
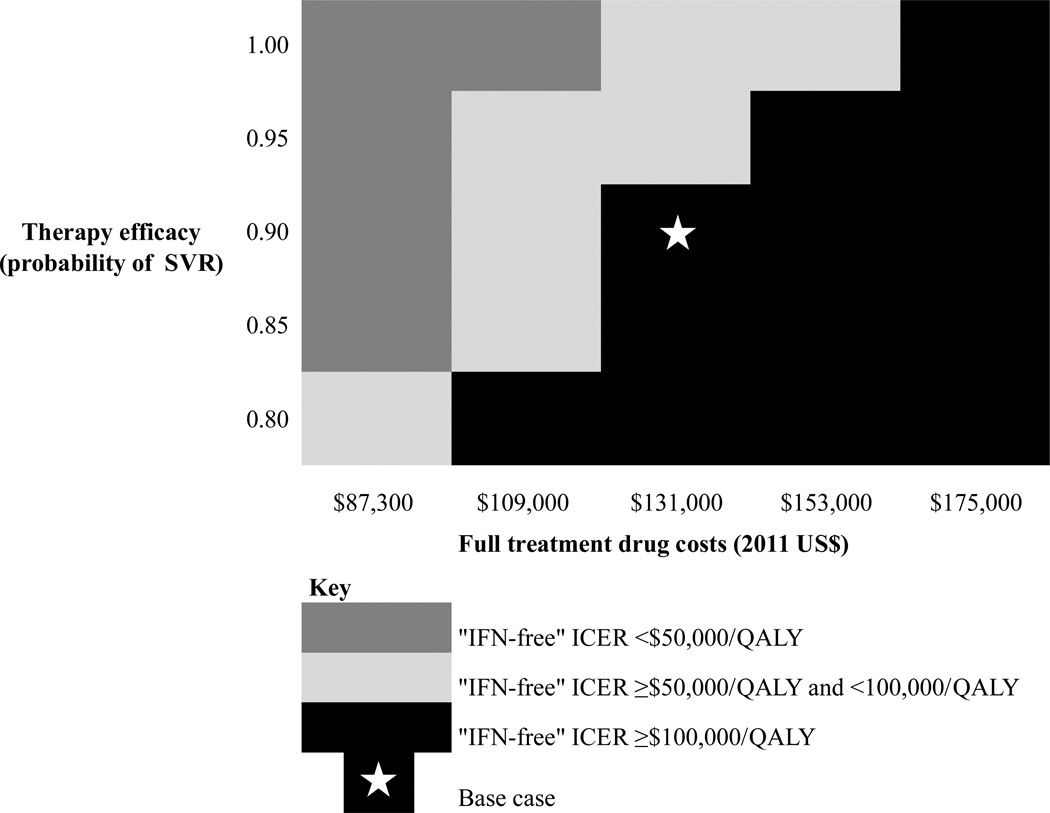
Results: 'PEG/RBV trial,' 'IL28B triage,' and 'triple therapy' each provided 72% SVR and extended QALE compared with 'dual therapy' by 1.12, 1.14, and 1.15 QALY, respectively. The ICER of 'PEG/RBV trial' compared with 'dual therapy' was $37 500/QALY. 'IL28B triage' and 'triple therapy' provided little benefit compared with 'PEG/RBV trial,' and both had ICERs exceeding $300 000/QALY. In sensitivity analyses, IFN-free treatment attaining 90% SVR had an ICER less than $100 000/QALY compared with 'PEG/RBV trial' when its cost was $109 000 or less (125% of the cost of PEG/RBV/TVR).
Conclusion: HCV protease inhibitors are most efficiently used in HIV/HCV coinfection after a trial of PEG/RBV, sparing protease inhibitors for those who attain rapid virologic response and SVR. The cost-effectiveness of IFN-free regimens for HIV/HCV coinfection will depend on the cost of these therapies.
Figures
References
-
- Ingiliz P, Rockstroh JK. HIV-HCV co-infection facing HCV protease inhibitor licensing: implications for clinicians. Liver Int. 2012;32:1194–1199. - PubMed
-
- Food and Drug Administration. [Accessed July 10, 2013];Approval of Incivek (TVRaprevir), a direct acting antiviral drug (DAA) to treat hepatitis C (HCV) From: http://www.fda.gov/ForConsumers/ByAudience/ForPatientAdvocates/ucm256328....
-
- Sulkowski MS, Sherman KE, Dieterich DT, Bsharat M, Mahnke L, Rockstroh JK, et al. Combination Therapy With TVRaprevir for Chronic Hepatitis C Virus Genotype 1 Infection in Patients With HIV: A Randomized Trial. Ann Intern Med. 2013;159:86–96. - PubMed
-
- Sulkowski M, Pol S, Mallolas J, Fainboim H, Cooper C, Slim J, et al. Boceprevir versus placebo with pegylated interferon alfa-2b and ribavirin for treatment of hepatitis C virus genotype 1 in patients with HIV: a randomised, double-blind, controlled phase 2 trial. Lancet Infect Dis. 2013;13:597–605. - PubMed
-
- Gilead Sciences. [Accessed July 10th, 2013];Gilead Submits New Drug Application to U.S. FDA for Sofosbuvir for the Treatment of Hepatitis C. from: http://investors.gilead.com/phoenix.zhtml?c=69964&p=irol-newsArticle&id=....
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
