

Phagocytosis via complement or Fc-gamma receptors is compromised in monocytes from type 2 diabetes patients with chronic hyperglycemia
- PMID: 24671137
- PMCID: PMC3966862
- DOI: 10.1371/journal.pone.0092977
Phagocytosis via complement or Fc-gamma receptors is compromised in monocytes from type 2 diabetes patients with chronic hyperglycemia
Abstract
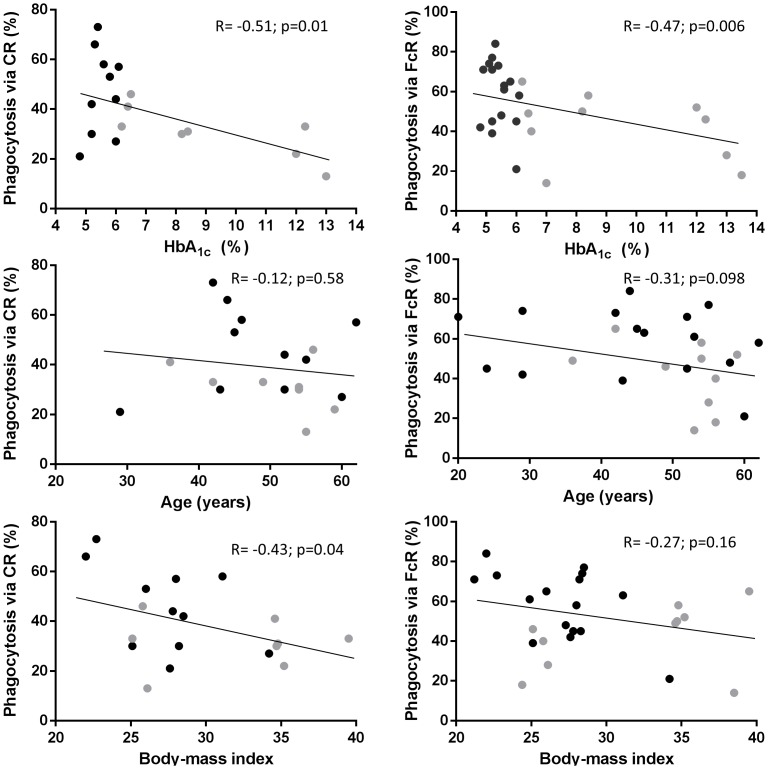
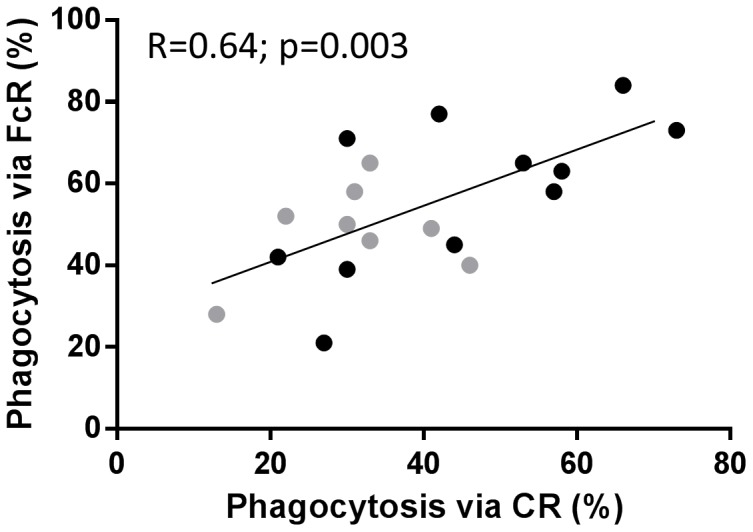
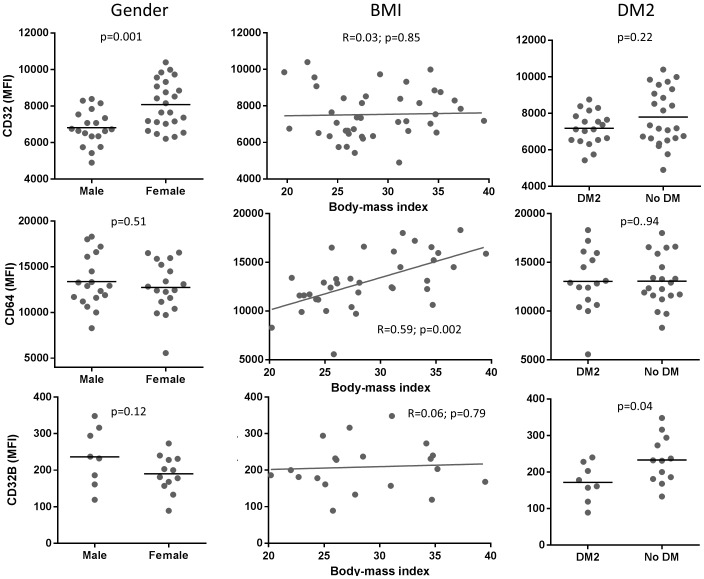
Type 2 diabetes patients (DM2) have a higher risk of tuberculosis (TB) that may be attributed to functional defects in their mononuclear phagocytes given the critical role of these cells in Mycobacterium tuberculosis containment. Our previous findings suggest that monocytes from DM2 have reduced association with serum-opsonized M. tuberculosis. To determine if this alteration is due to defects in phagocytosis via complement or Fc-gamma receptors (FcγRs), in this study we evaluated the uptake of sheep red blood cells coated with IgG or complement, respectively, by monocytes from individuals with and without DM2. We found that chronic hyperglycemia was significantly associated with reduced phagocytosis via either receptor by univariable and multivariable analyses. This defect was independent of host serum opsonins and flow cytometry data indicated this was not attributed to reduced expression of these phagocytic receptors on DM2 monocytes. The positive correlation between both pathways (R = 0.64; p = 0.003) indicate that monocytes from individuals with chronic hyperglycemia have a defect in the two predominant phagocytic pathways of these cells. Given that phagocytosis is linked to activation of effector mechanisms for bacterial killing, it is likely that this defect is one factor contributing to the higher susceptibility of DM2 patients to pathogens like M. tuberculosis.
Conflict of interest statement
Figures
References
-
- Peleg AY, Weerarathna T, McCarthy JS, Davis TM (2007) Common infections in diabetes: pathogenesis, management and relationship to glycaemic control. Diabetes Metab Res Rev 23: 3–13. - PubMed
-
- Zumla A, Raviglione M, Hafner R, von Reyn CF (2013) Tuberculosis. N Engl J Med 368: 745–755. - PubMed
-
- World Health Organization (2013) Global tuberculosis report 2013. Available: http://apps.who.int/iris/bitstream/10665/91355/1/9789241564656_eng.pdf.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
