

Case Reports
doi: 10.1136/bcr-2013-202939.
Treating neuromyelitis optica with the interleukin-6 receptor antagonist tocilizumab
Affiliations
- PMID: 24671322
- PMCID: PMC3975485
- DOI: 10.1136/bcr-2013-202939
Item in Clipboard
Case Reports
Treating neuromyelitis optica with the interleukin-6 receptor antagonist tocilizumab
BMJ Case Rep.
.
Abstract
We present a 32-year-old female patient with fulminant neuromyelitis optica. After the initial treatment with the monoclonal antibody rituximab failed, therapy with the anti-IL-6 receptor antagonist tocilizumab was initiated. The patient experienced a clinically relevant improvement from severe tetraparesis to low-grade paresis, which is still maintained. On MRI of the spinal cord an almost complete restitution of a predescribed extensive myelopathy accompanied this clinical improvement. Meanwhile clinical stability was achieved for over 1 year without any side effects of the ongoing treatment with tocilizumab.
Figures
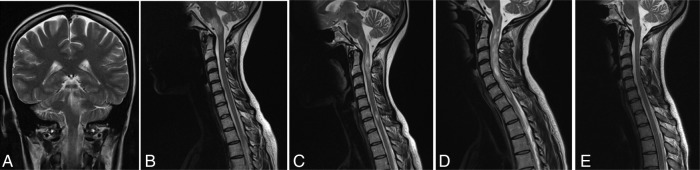
(A) Cranial MRI in January 2010 revealed lesion of the periaqueductal grey with extension to the left cerebellar hemisphere as well as to the pons and the medulla oblongata on T2-weighted images, after a new attack presenting as bilateral internuclear ophthalmoplegia, crossed brainstem symptoms, nausea and intractable hiccups. (B) Spinal MRI in July 2010 showed a newly occurred T2 hyperintense lesion that affected almost the entire cross-section of the medulla oblongata and the pons, causative for a new relapse with brainstem symptoms. (C) T2-weighted spinal cord MRI in July 2012, when the patient presented with sensory disturbances, revealed multiple circumscribed hyperintense lesions, the cranial one extending over two vertebral segments. (D) Spinal cord MRI in October 2012 after a severe clinical deterioration to an Expanded Disability Status Scale of 9 demonstrated an extensive myelopathy from cervical vertebra 1 to 7. (E) MRI in August 2013 showed an almost complete restitution of the previously described myelopathy on T2-weighted images, after 10 months treated with tocilizumab.

Clinical course and concomitant drugs.NTZ: natalizumab 300 mg monthly; PLEX: plasmaexchange; RTX: rituximab 2×1000 mg; TCZ: tocilizumab 8 mg/kg body weight monthly.
References
-
- Wingerchuk DM, Lennon VA, Pittock SJ, et al. Revised diagnostic criteria for neuromyelitis optica. Neurology 2006;66:1485–9 - PubMed
-
- Weinstock-Guttman B, Ramanathan M, Lincoff N, et al. Study of mitoxantrone for the treatment of recurrent neuromyelitis optica (Devic disease). Arch Neurol 2006;63:957–63 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials