

The burden of gastrointestinal anastomotic leaks: an evaluation of clinical and economic outcomes
- PMID: 24671472
- PMCID: PMC4028541
- DOI: 10.1007/s11605-014-2506-4
The burden of gastrointestinal anastomotic leaks: an evaluation of clinical and economic outcomes
Abstract
Objective: To evaluate the clinical and economic burden associated with anastomotic leaks following colorectal surgery.
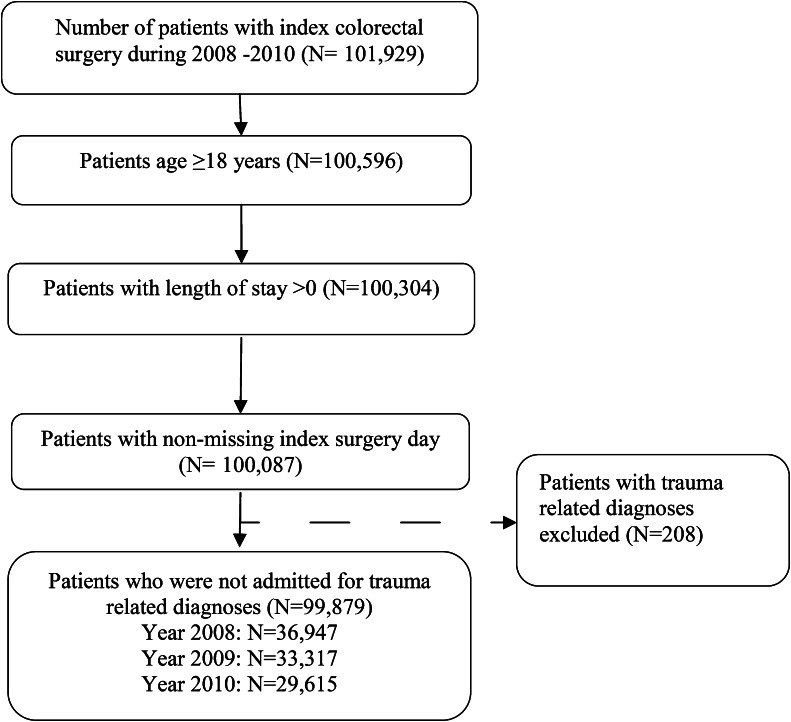
Methods: Retrospective data (January 2008 to December 2010) were analyzed from patients who had colorectal surgery with and without postoperative leaks, using the Premier Perspective™ database. Data on in-hospital mortality, length of stay (LOS), re-admissions, postoperative infection, and costs were analyzed using univariate and multivariate analyses, and the propensity score matching (PSM) and generalized linear models (GLM).
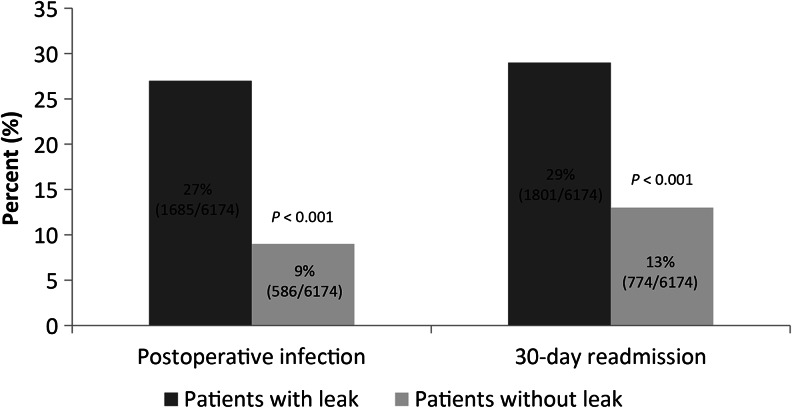
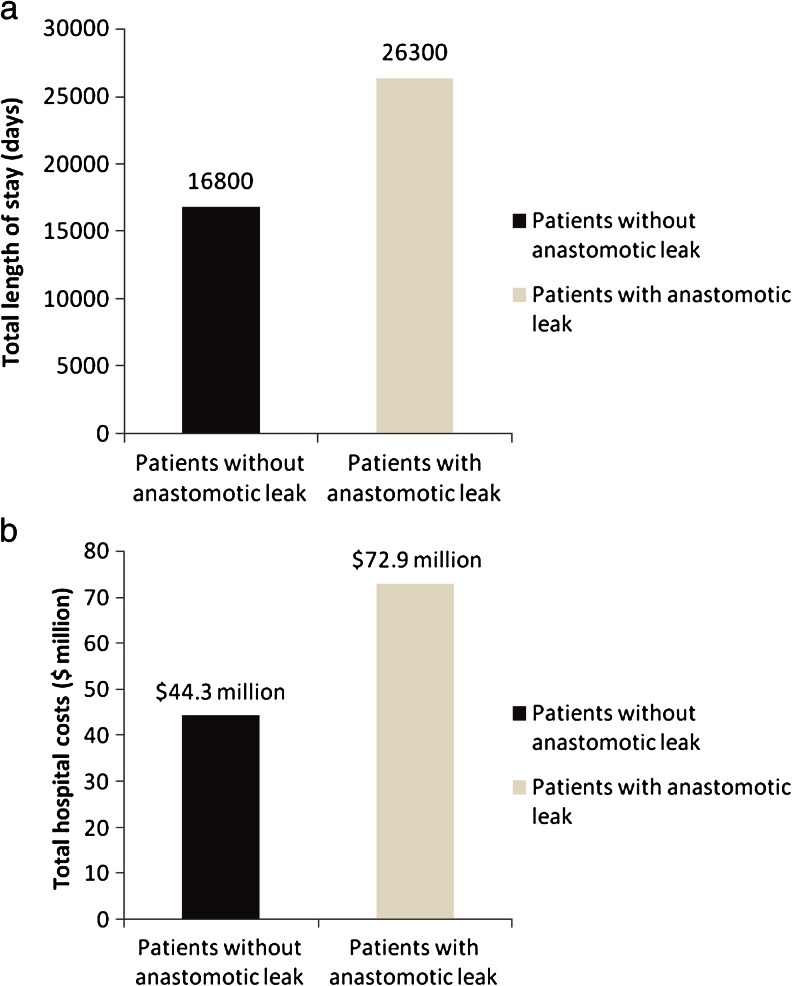
Results: Of the patients, 6,174 (6.18 %) had anastomotic leaks within 30 days after colorectal surgery. Patients with leaks had 1.3 times higher 30-day re-admission rates and 0.8-1.9 times higher postoperative infection rates as compared with patients without leaks (P < 0.001 for both). Anastomotic leaks incurred additional LOS and hospital costs of 7.3 days and $24,129, respectively, only within the first hospitalization. Per 1,000 patients undergoing colorectal surgery, the economic burden associated with anastomotic leaks--including hospitalization and re-admission--was established as 9,500 days in prolonged LOS and $28.6 million in additional costs. Similar results were obtained from both the PSM and GLM for assessing total costs for hospitalization and re-admission.
Conclusions: Anastomotic leaks in colorectal surgery increase the total clinical and economic burden by a factor of 0.6-1.9 for a 30-day re-admission, postoperative infection, LOS, and hospital costs.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
