

Therapeutic modalities for Pancoast tumors
- PMID: 24672693
- PMCID: PMC3966148
- DOI: 10.3978/j.issn.2072-1439.2013.12.31
Therapeutic modalities for Pancoast tumors
Abstract
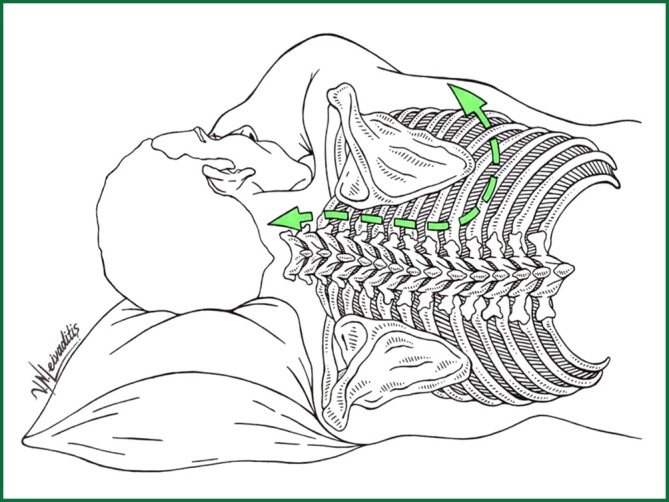
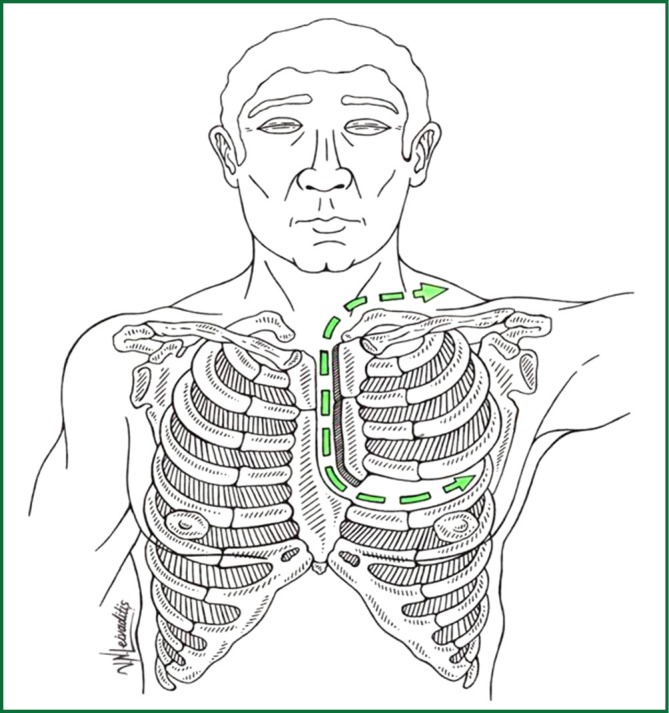
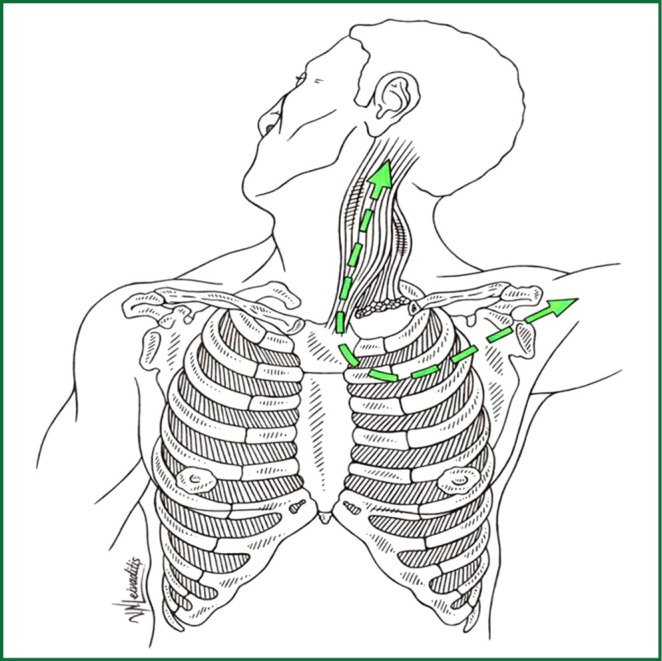
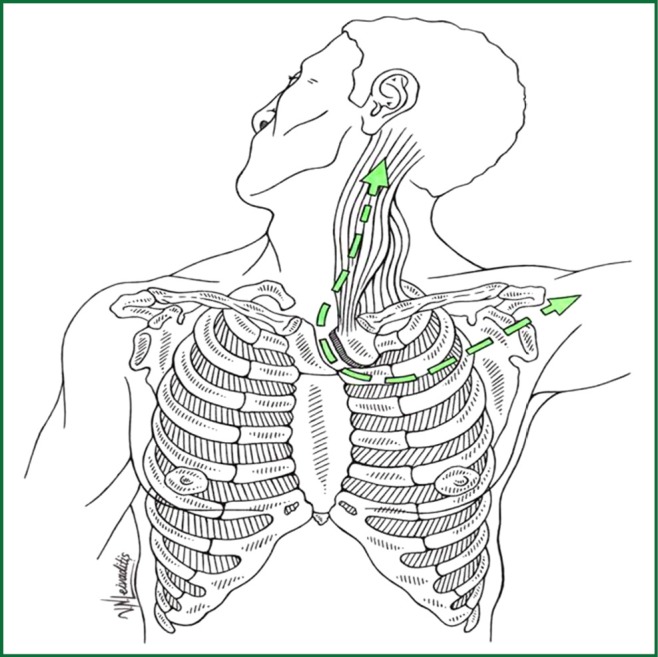
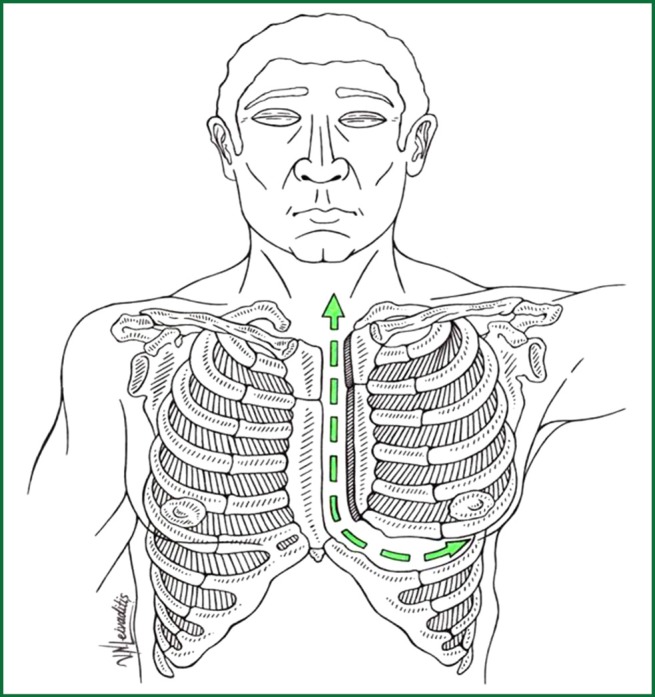
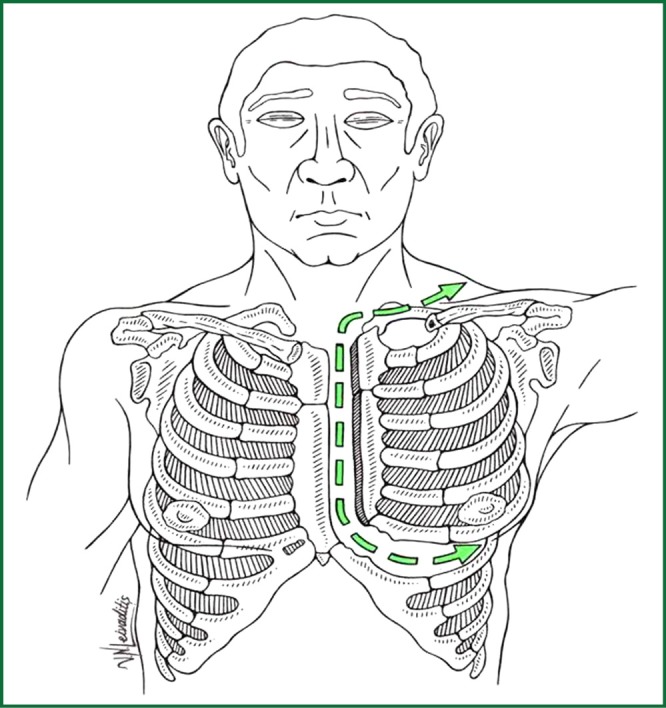
A Pancoast tumor, also called a pulmonary sulcus tumor or superior sulcus tumor, is a tumor of the pulmonary apex. It is a type of lung cancer defined primarily by its location situated at the top end of either the right or left lung. It typically spreads to nearby tissues such as the ribs and vertebrae. Most Pancoast tumors are non-small cell cancers. The growing tumor can cause compression of a brachiocephalic vein, subclavian artery, phrenic nerve, recurrent laryngeal nerve, vagus nerve, or, characteristically, compression of a sympathetic ganglion resulting in a range of symptoms known as Horner's syndrome. Pancoast tumors are named for Henry Pancoast, a US radiologist, who described them in 1924 and 1932.The treatment of a Pancoast lung cancer may differ from that of other types of non-small cell lung cancer (NSCLC). Its position and close proximity to vital structures may make surgery difficult. As a result, and depending on the stage of the cancer, treatment may involve radiation and chemotherapy given prior to surgery. Surgery may consist of the removal of the upper lobe of a lung together with its associated structures as well as mediastinal lymphadenectomy. Surgical access may be via thoracotomy from the back or the front of the chest and modification. Careful patient selection, improvements in imaging such as the role of PET-CT in restaging of tumors, radiotherapy and surgical advances, the management of previously inoperable lesions by a combined experienced thoracic-neurosurgical team and prompt recognition and therapy of postoperative complications has greatly increased local control and overall survival for patients with these tumors.
Keywords: Pancoast; lung cancer; therapy.
Figures
References
-
- Chardack WM, Maccallum JD. Pancoast syndrome due to bronchiogenic carcinoma: successful surgical removal and postoperative irradiation; a case report. J Thorac Surg 1953;25:402-12 - PubMed
-
- Shahian DM. Contemporary management of superior pulmonary sulcus (Pancoast) lung tumors. Curr Opin Pulm Med 2003;9:327-31 - PubMed
-
- Wright CD, Menard MT, Wain JC, et al. Induction chemoradiation compared with induction radiation for lung cancer involving the superior sulcus. Ann Thorac Surg 2002;73:1541-4 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous