

Neuropathological staging of spinocerebellar ataxia type 2 by semiquantitative 1C2-positive neuron typing. Nuclear translocation of cytoplasmic 1C2 underlies disease progression of spinocerebellar ataxia type 2
- PMID: 24674145
- PMCID: PMC8028922
- DOI: 10.1111/bpa.12146
Neuropathological staging of spinocerebellar ataxia type 2 by semiquantitative 1C2-positive neuron typing. Nuclear translocation of cytoplasmic 1C2 underlies disease progression of spinocerebellar ataxia type 2
Abstract
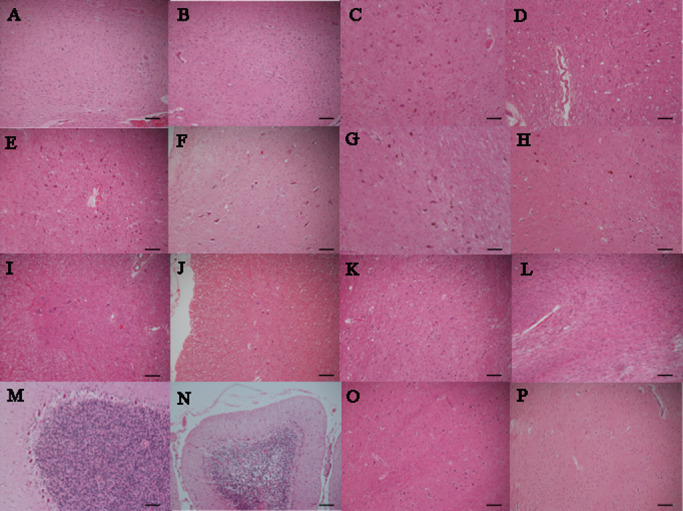
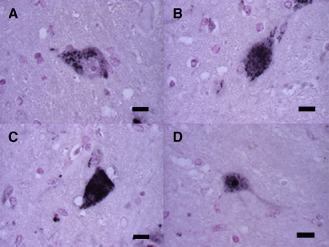
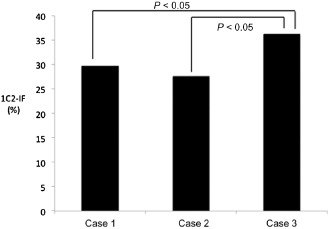
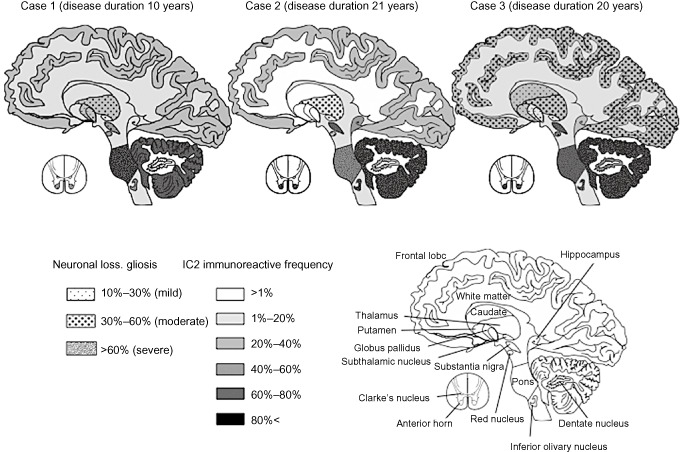
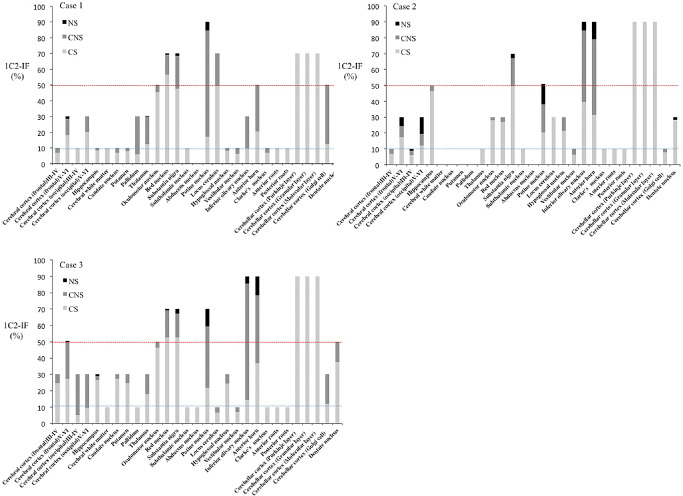
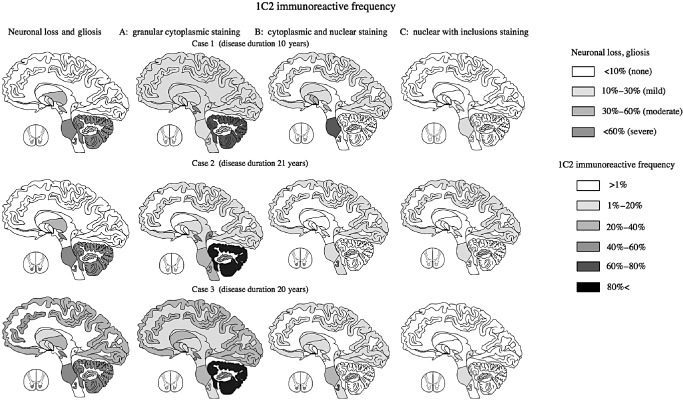
Spinocerebellar ataxia type 2 (SCA2) is a hereditary neurodegenerative disorder caused by the expansion of the trinucleotide CAG repeats encoding elongated polyglutamine tract in ataxin-2, the SCA2 gene product. Polyglutamine diseases comprise nine genetic entities, including seven different forms of spinocerebellar ataxias, Huntington's disease, and spinal and bulbar muscular atrophy. These are pathologically characterized by neuronal loss and intranuclear aggregates or inclusions of mutant proteins including expanded polyglutamine in selected neuronal groups. Previously, we examined immunolocalization of ubiquitin, expanded polyglutamine (probed by 1C2 antibody), and ataxin-2 in genetically confirmed SCA2 patients. In the present study, we expanded this approach by distinguishing different patterns of subcellular 1C2 immunoreactivity ("granular cytoplasmic," "cytoplasmic and nuclear" and "nuclear with inclusions.") and by quantifying their regional frequencies in three autopsied SCA2 brains at different stage of the disease. Comparison with neuronal loss and gliosis revealed that overall 1C2 immunoreactivity was paralleled with their severity. Furthermore, appearance of granular cytoplasmic pattern corresponded to early stage, cytoplasmic and nuclear pattern to active stage, and nuclear with inclusions pattern to final stage. We conclude that this 1C2-immunoreactive typing may be useful for evaluating the overall severity and extent of affected regions and estimating the neuropathological stage of SCA2.
Keywords: 1C2-immunoreactive typing; cytoplasmic and nuclear; granular cytoplasmic; nuclear with inclusions; spinocerebellar ataxia type 2.
© 2014 International Society of Neuropathology.
Figures
Similar articles
-
On the distribution of intranuclear and cytoplasmic aggregates in the brainstem of patients with spinocerebellar ataxia type 2 and 3.Brain Pathol. 2017 May;27(3):345-355. doi: 10.1111/bpa.12412. Epub 2016 Aug 2. Brain Pathol. 2017. PMID: 27377427 Free PMC article.
-
Parallel Appearance of Polyglutamine and Transactivation-Responsive DNA-Binding Protein 43 and Their Complementary Subcellular Localization in Brains of Patients With Spinocerebellar Ataxia Type 2.J Neuropathol Exp Neurol. 2022 Jun 20;81(7):535-544. doi: 10.1093/jnen/nlac032. J Neuropathol Exp Neurol. 2022. PMID: 35511239
-
Neuronal intranuclear inclusions in spinocerebellar ataxia type 2: triple-labeling immunofluorescent study.Neurosci Lett. 1999 Oct 1;273(2):117-20. doi: 10.1016/s0304-3940(99)00656-4. Neurosci Lett. 1999. PMID: 10505630
-
Spinocerebellar ataxia 2 (SCA2).Cerebellum. 2008;7(2):115-24. doi: 10.1007/s12311-008-0019-y. Cerebellum. 2008. PMID: 18418684 Review.
-
An autopsy case of an aged patient with spinocerebellar ataxia type 2.Neuropathology. 2011 Oct;31(5):510-8. doi: 10.1111/j.1440-1789.2010.01176.x. Epub 2010 Dec 6. Neuropathology. 2011. PMID: 21134000 Review.
Cited by
-
Substantia nigra degeneration in spinocerebellar ataxia 2 and 7 using neuromelanin-sensitive imaging.Eur J Neurol. 2025 Jan;32(1):e70035. doi: 10.1111/ene.70035. Eur J Neurol. 2025. PMID: 39757380 Free PMC article.
-
From pathways to targets: understanding the mechanisms behind polyglutamine disease.Biomed Res Int. 2014;2014:701758. doi: 10.1155/2014/701758. Epub 2014 Sep 21. Biomed Res Int. 2014. PMID: 25309920 Free PMC article. Review.
-
Interrupted CAG expansions in ATXN2 gene expand the genetic spectrum of frontotemporal dementias.Acta Neuropathol Commun. 2018 May 30;6(1):41. doi: 10.1186/s40478-018-0547-8. Acta Neuropathol Commun. 2018. PMID: 29848387 Free PMC article. No abstract available.
-
ATXN2 is a target of N-terminal proteolysis.PLoS One. 2023 Dec 21;18(12):e0296085. doi: 10.1371/journal.pone.0296085. eCollection 2023. PLoS One. 2023. PMID: 38128014 Free PMC article.
-
Autophagy in Spinocerebellar ataxia type 2, a dysregulated pathway, and a target for therapy.Cell Death Dis. 2021 Nov 29;12(12):1117. doi: 10.1038/s41419-021-04404-1. Cell Death Dis. 2021. PMID: 34845184 Free PMC article.
References
-
- Armstrong J, Bonaventura I, Rojo A, González G, Corral J, Nadal N et al (2005) Spinocerebellar ataxia type 2 (SCA2) with white matter involvement. Neurosci Lett 381:247–251. - PubMed
-
- Arrasate M, Mitra S, Schweitzer ES, Segal MR, Finkbeiner S (2004) Inclusion body formation reduces levels of mutant Huntington and the risk of neuronal death. Nature 431:805–810. - PubMed
-
- Dürr A, Smadja D, Cancel G, Lezin A, Stevanin G, Mikol J et al (1995) Autosomal dominant cerebellar ataxia type I in Martinique (French West Indies). Clinical and neuropathological analysis of 53 patients from three unrelated SCA2 families. Brain 118:1573–1581. - PubMed
-
- Fujigasaki H, Uchihara T, Koyano S, Iwabuchi K, Yagishita S, Makifuchi T et al (2000) Ataxin‐3 is translocated into the nucleus for the formation of intranuclear inclusions in normal and Machado‐Joseph disease brains. Exp Neurol 165:248–256. - PubMed
-
- Gierga K, Bürk K, Bauer M, Orozco Diaz G, Auburger G, Schultz C et al (2005) Involvement of the cranial nerves and their nuclei in spinocerebellar ataxia type 2 (SCA2). Acta Neuropathol 109:617–631. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
