

Low uptake of colorectal cancer screening among African Americans in an integrated Veterans Affairs health care network
- PMID: 24674351
- PMCID: PMC4104145
- DOI: 10.1016/j.gie.2014.01.045
Low uptake of colorectal cancer screening among African Americans in an integrated Veterans Affairs health care network
Abstract
Background: African Americans have the highest incidence and mortality from colorectal cancer (CRC). Despite guidelines to initiate screening with colonoscopy at age 45 in African Americans, the CRC incidence remains high in this group.
Objective: To examine the rates and predictors of CRC screening uptake as well as time to screening in a population of African Americans and non-African Americans in a health care system that minimizes variations in insurance and access.
Design: Retrospective cohort study.
Setting: Greater Los Angeles Veterans Affairs (VA) Healthcare System.
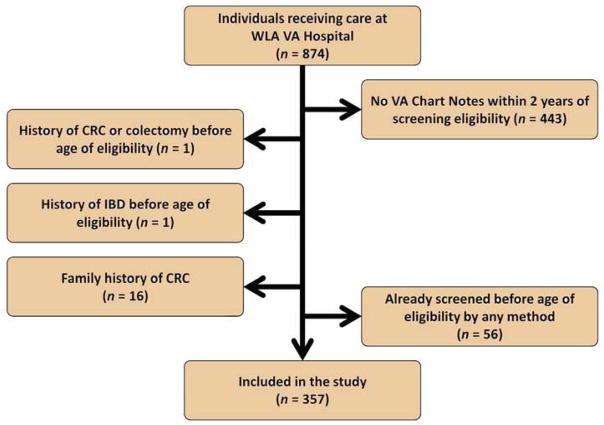
Patients: Random sample (N = 357) of patients eligible for initial CRC screening.
Main outcome measurements: Uptake of any screening method; uptake of colonoscopy, in particular; predictors of screening; and time to screening in African Americans and non-African Americans.
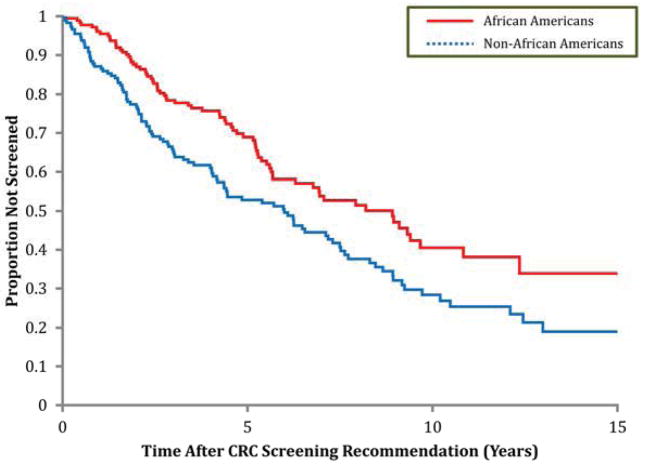
Results: The overall screening rate by any method was 50%. Adjusted rates for any screening were lower among African Americans than non-African Americans (42% vs 58%; odds ratio [OR] 0.49; 95% confidence interval [CI], 0.31-0.77). Colonoscopic screening was also lower in African Americans (11% vs 23%; adjusted OR 0.43; 95% CI, 0.24-0.77). In addition to race, homelessness, lower service connectedness, taking more prescription drugs, and not seeing a primary care provider within 2 years of screening eligibility predicted lower uptake of screening. Time to screening colonoscopy was longer in African Americans (adjusted hazard ratio 0.43; 95% CI, 0.25-0.75).
Limitations: The sample may not be generalizable.
Conclusions: We found marked disparities in CRC screening despite similar access to care across races. Despite current guidelines aimed at increasing CRC screening in African Americans, participation in screening remained low, and use of colonoscopy was infrequent.
Published by Mosby, Inc.
Figures
References
-
- American Cancer Society. Colorectal cancer facts & figures 2011–2013. Atlanta, GA:
-
- Agrawal S, et al. Colorectal cancer in African Americans. Am J Gastroenterol. 2005;100(3):515–23. discussion 514. - PubMed
-
- Baquet CR, Commiskey P. Colorectal cancer epidemiology in minorities: a review. J Assoc Acad Minor Phys. 1999;10(3):51–8. - PubMed
-
- Butler LM, et al. Heterocyclic amines, meat intake, and association with colon cancer in a population-based study. Am J Epidemiol. 2003;157(5):434–45. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
