

Effects of antimicrobial prophylaxis and blood stream infections in patients with acute liver failure: a retrospective cohort study
- PMID: 24674942
- PMCID: PMC4205208
- DOI: 10.1016/j.cgh.2014.03.011
Effects of antimicrobial prophylaxis and blood stream infections in patients with acute liver failure: a retrospective cohort study
Abstract
Background & aims: We investigated whether antimicrobial prophylaxis alters the incidence of bloodstream infection in patients with acute liver failure (ALF), and whether bloodstream infections affect overall mortality within 21 days after development of ALF.
Methods: We performed a retrospective cohort analysis of 1551 patients with ALF enrolled by the US Acute Liver Failure Study Group from January 1998 through November 2009. We analyzed data on infections in the first 7 days after admission and the effects of prophylaxis with antimicrobial drugs on the development of bloodstream infections and 21-day mortality.
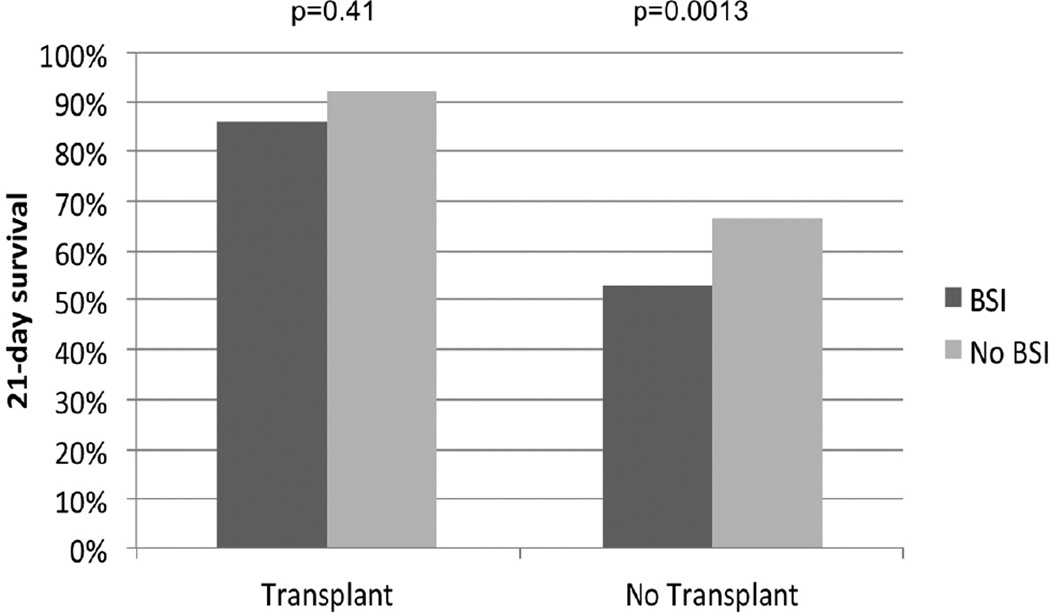
Results: In our study population, 600 patients (39%) received antimicrobial prophylaxis and 226 patients (14.6%) developed at least 1 bloodstream infection. Exposure to antimicrobial drugs did not affect the proportion of patients who developed bloodstream infections (12.8% in patients with prophylaxis vs 15.7% in nonprophylaxed patients; P = .12), but a greater percentage of patients who received prophylaxis received liver transplants (28% vs 22%; P = .01). After adjusting for confounding factors, overall mortality within 21 days was associated independently with age (odds ratio [OR], 1.014), Model for End-stage Liver Disease score at admission (OR, 1.078), and vasopressor administration at admission (OR, 2.499). Low grade of coma (OR, 0.47) and liver transplantation (OR, 0.101) reduced mortality. Although bloodstream infection was associated significantly with 21-day mortality (P = .004), an interaction between bloodstream infection and etiology was detected: blood stream infection affected mortality to a greater extent in nonacetaminophen ALF patients (OR, 2.03) than in acetaminophen ALF patients (OR, 1.14).
Conclusions: Based on a large, observational study, antimicrobial prophylaxis does not reduce the incidence of bloodstream infection or mortality within 21 days of ALF. However, bloodstream infections were associated with increased 21-day mortality in patients with ALF-to a greater extent in patients without than with acetaminophen-associated ALF. Our findings do not support the routine use of antimicrobial prophylaxis in patients with ALF.
Keywords: APAP; Antibiotic; Compensatory Anti-inflammatory Response Syndrome; Liver Damage; Systemic Inflammatory Response Syndrome.
Copyright © 2014 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Antibiotic prophylaxis in acute liver failure: friend or foe?Clin Gastroenterol Hepatol. 2014 Nov;12(11):1950-2. doi: 10.1016/j.cgh.2014.05.008. Epub 2014 May 16. Clin Gastroenterol Hepatol. 2014. PMID: 24842669 No abstract available.
References
-
- Antoniades CG, Berry PA, Wendon JA, et al. The importance of immune dysfunction in determining outcome in acute liver failure. J Hepatol. 2008;49:845–861. - PubMed
-
- Calandra T, Gerain J, Heumann D, et al. High circulating levels of interleukin-6 in patients with septic shock: evolution during sepsis, prognostic value, and interplay with other cytokines. The Swiss-Dutch J5 Immunoglobulin Study Group. Am J Med. 1991;91:23–29. - PubMed
-
- Martin C, Boisson C, Haccoun M, et al. Patterns of cytokine evolution (tumor necrosis factor-alpha and interleukin-6) after septic shock, hemorrhagic shock, and severe trauma. Crit Care Med. 1997;25:1813–1819. - PubMed
-
- Friedman G, Jankowski S, Marchant A, et al. Blood interleukin 10 levels parallel the severity of septic shock. J Crit Care. 1997;12:183–187. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
