

Urinary TIMP-2 and IGFBP7 as early biomarkers of acute kidney injury and renal recovery following cardiac surgery
- PMID: 24675717
- PMCID: PMC3968141
- DOI: 10.1371/journal.pone.0093460
Urinary TIMP-2 and IGFBP7 as early biomarkers of acute kidney injury and renal recovery following cardiac surgery
Abstract
Background: Difficulties in prediction and early identification of (acute kidney injury) AKI have hindered the ability to develop preventive and therapeutic measures for this syndrome. We tested the hypothesis that a urine test measuring insulin-like growth factor-binding protein 7 (IGFBP7) and tissue inhibitor of metalloproteinases-2 (TIMP-2), both inducers of G1 cell cycle arrest, a key mechanism implicated in acute kidney injury (AKI), could predict AKI in cardiac surgery patients.
Methods: We studied 50 patients at high risk for AKI undergoing cardiac surgery with cardiopulmonary bypass (CPB). Serial urine samples were analyzed for [TIMP-2]*[IGFBP7] concentrations. The primary outcome measure was AKI as defined by international consensus criteria following surgery. Furthermore, we investigated whether urine [TIMP-2]*[IGFBP7] could predict renal recovery from AKI prior to hospital discharge.
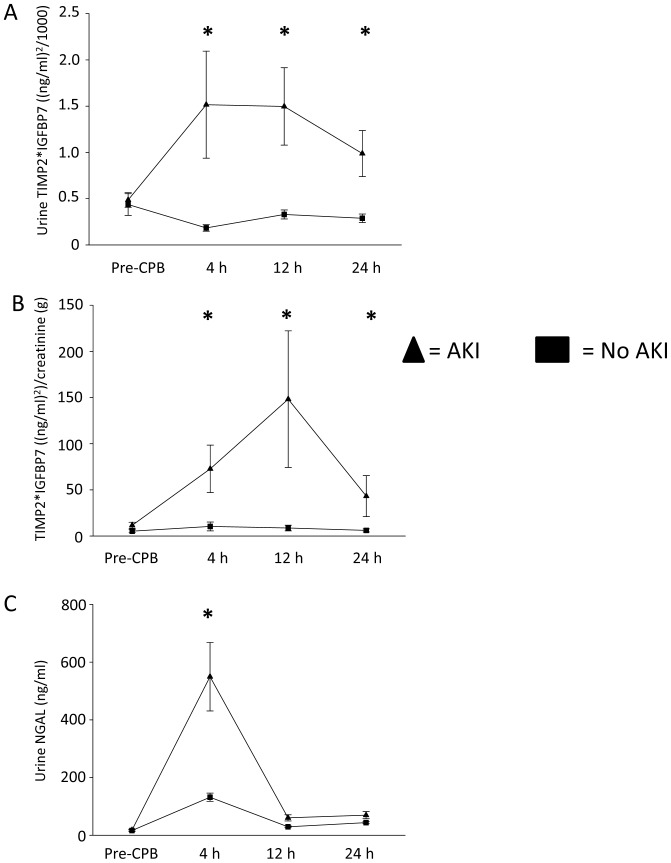
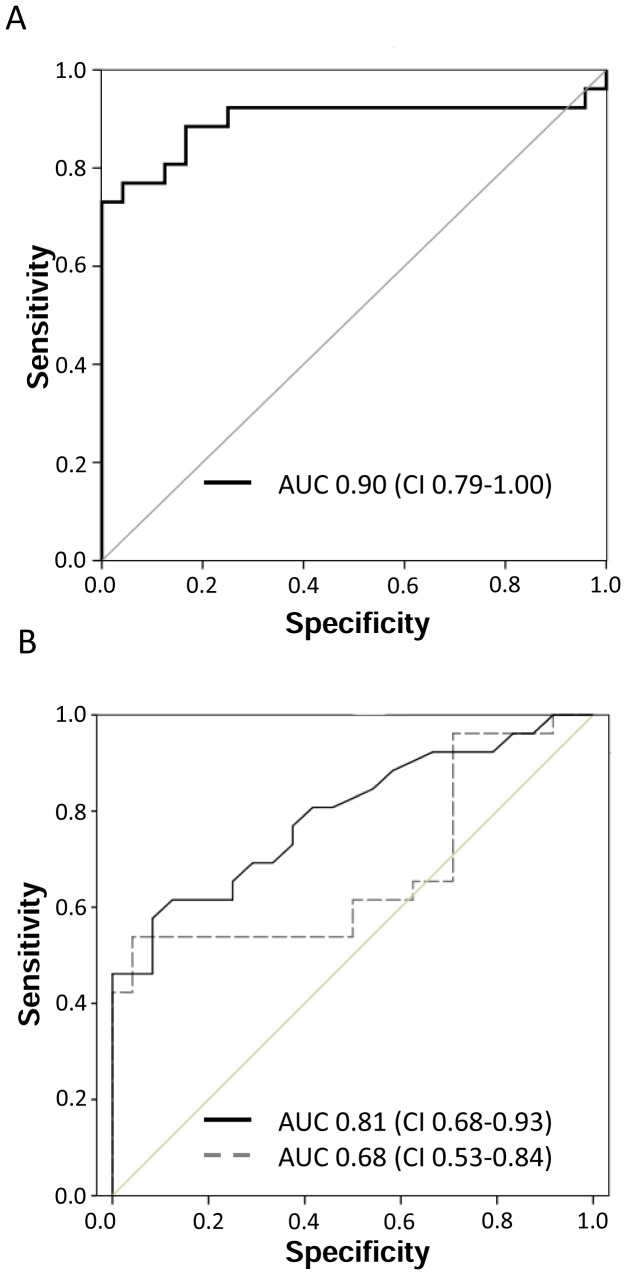
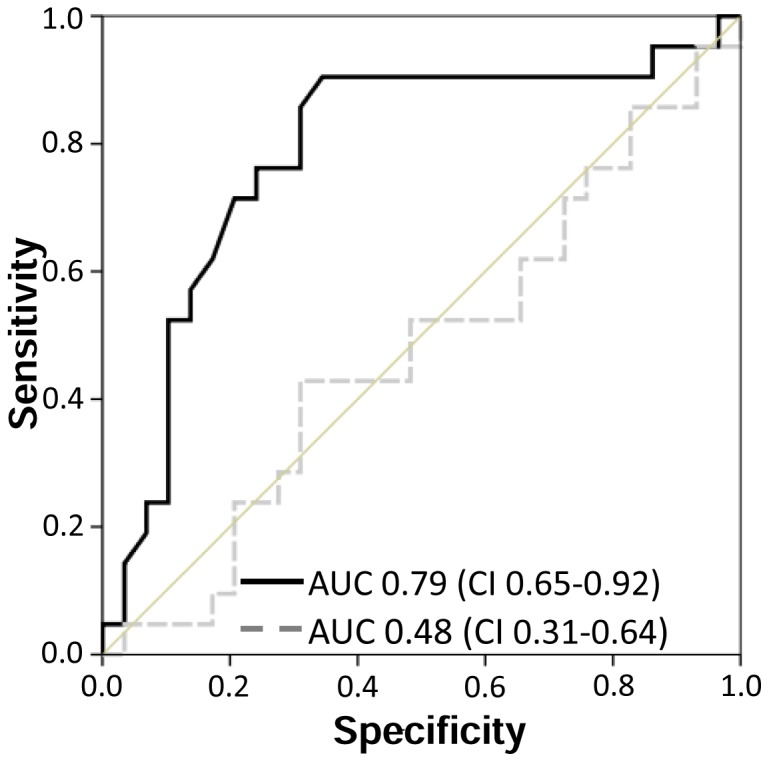
Results: 26 patients (52%) developed AKI. Diagnosis based on serum creatinine and/or oliguria did not occur until 1-3 days after CPB. In contrast, urine concentration of [TIMP-2]*[IGFBP7] rose from a mean of 0.49 (SE 0.24) at baseline to 1.51 (SE 0.57) 4 h after CPB in patients who developed AKI. The maximum urinary [TIMP-2]*[IGFBP7] concentration achieved in the first 24 hours following surgery (composite time point) demonstrated an area under the receiver-operating characteristic curve of 0.84. Sensitivity was 0.92, and specificity was 0.81 for a cutoff value of 0.50. The decline in urinary [TIMP-2]*[IGFBP7] values was the strongest predictor for renal recovery.
Conclusions: Urinary [TIMP-2]*[IGFBP7] serves as a sensitive and specific biomarker to predict AKI early after cardiac surgery and to predict renal recovery.
Clinical trial registration information: www.germanctr.de/, DRKS-ID: DRKS00005062.
Conflict of interest statement
Figures
References
-
- Wijeysundera DN, Karkouti K, Dupuis JY, Rao V, Chan CT, et al. (2007) Derivation and validation of a simplified predictive index for renal replacement therapy after cardiac surgery. JAMA 297: 1801–1809. - PubMed
-
- Chertow GM, Levy EM, Hammermeister KE, Grover F, Daley J (1998) Independent association between acute renal failure and mortality following cardiac surgery. Am J Med 104: 343–348. - PubMed
-
- Mangano CM, Diamondstone LS, Ramsay JG, Aggarwal A, Herskowitz A, et al. (1998) Renal dysfunction after myocardial revascularization: risk factors, adverse outcomes, and hospital resource utilization. The Multicenter Study of Perioperative Ischemia Research Group. Ann Intern Med 128: 194–203. - PubMed
-
- Zanardo G, Michielon P, Paccagnella A, Rosi P, Calo M, et al. (1994) Acute renal failure in the patient undergoing cardiac operation. Prevalence, mortality rate, and main risk factors. J Thorac Cardiovasc Surg 107: 1489–1495. - PubMed
-
- Lassnigg A, Schmidlin D, Mouhieddine M, Bachmann LM, Druml W, et al. (2004) Minimal changes of serum creatinine predict prognosis in patients after cardiothoracic surgery: a prospective cohort study. J Am Soc Nephrol 15: 1597–1605. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
