

Community-based active tuberculosis case finding in poor urban settlements of Phnom Penh, Cambodia: a feasible and effective strategy
- PMID: 24675985
- PMCID: PMC3968028
- DOI: 10.1371/journal.pone.0092754
Community-based active tuberculosis case finding in poor urban settlements of Phnom Penh, Cambodia: a feasible and effective strategy
Abstract
Background: In light of the limitations of the current case finding strategies and the global urgency to improve tuberculosis (TB) case-detection, a renewed interest in active case finding (ACF) has risen. The WHO calls for more evidence on innovative ways of TB screening, especially from low-income countries, to inform global guideline development. We aimed to assess the feasibility of community-based ACF for TB among the urban poor in Cambodia and determine its impact on case detection, treatment uptake and outcome.
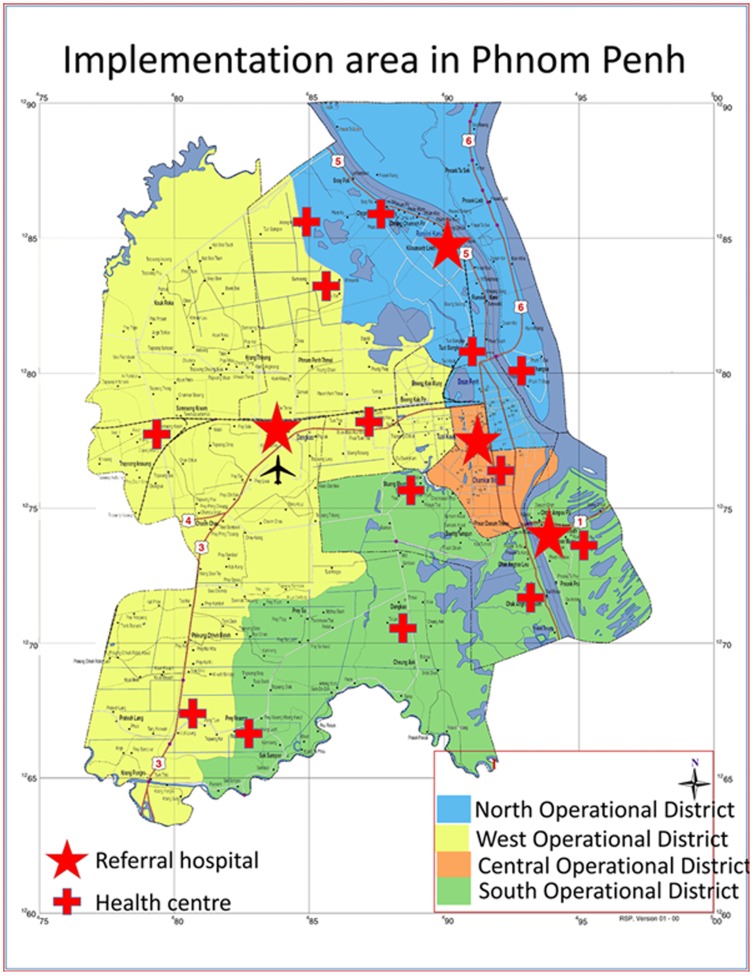
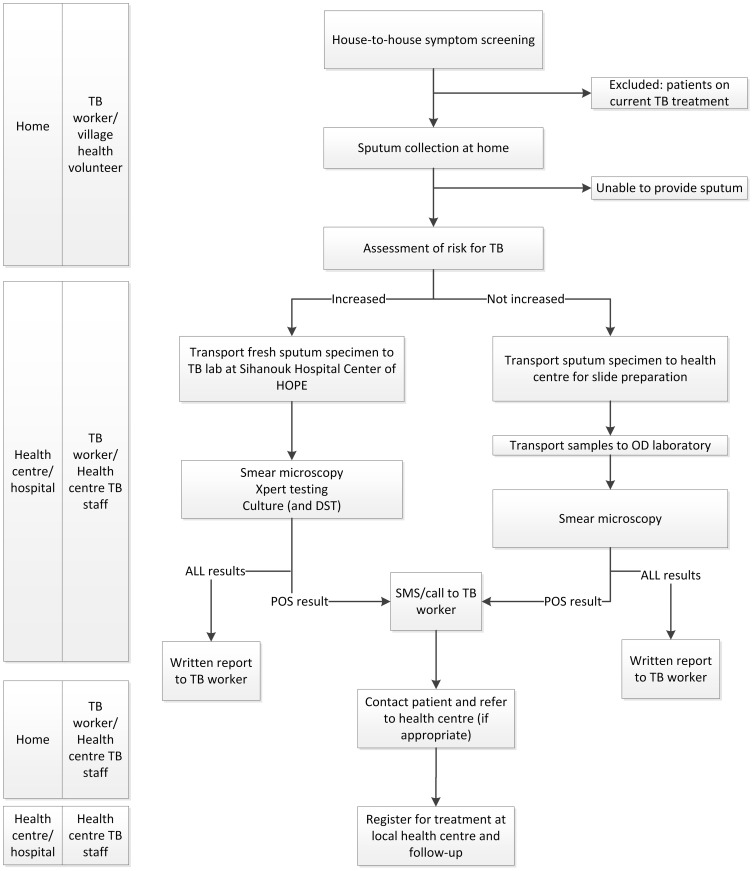
Methods: Between 9/2/2012-31/3/2013 the Sihanouk Hospital Center of HOPE conducted a door-to-door survey for TB in deprived communities of Phnom Penh. TB workers and community health volunteers performed symptom screening, collected sputum and facilitated specimen transport to the laboratories. Fluorescence microscopy was introduced at three referral hospitals. The GeneXpert MTB/RIF assay (Xpert) was performed at tertiary level for individuals at increased risk of HIV-associated, drug-resistant or smear-negative TB. Mobile phone/short message system (SMS) was used for same-day issuing of positive results. TB workers contacted diagnosed patients and referred them for care at their local health centre.
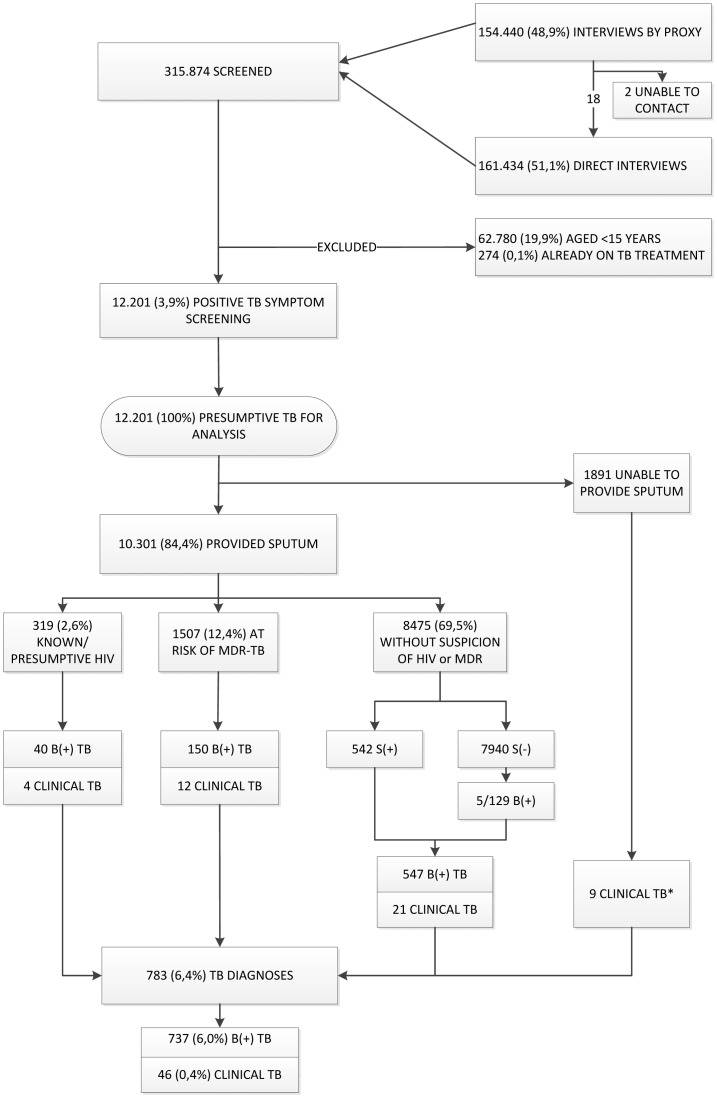
Results: In 14 months, we screened 315.874 individuals; we identified 12.201 aged ≥ 15 years with symptoms suggestive of TB; 84% provided sputum. We diagnosed 783, including 737 bacteriologically confirmed, TB cases. Xpert testing yielded 41% and 48% additional diagnoses among presumptive HIV-associated and multidrug-resistant TB cases, respectively. The median time from sputum collection to notification (by SMS) of the first positive (microscopy or Xpert) result was 3 days (IQR 2-6). Over 94% commenced TB treatment and 81% successfully completed it.
Conclusion: Our findings suggest that among the urban poor ACF for TB, using a sensitive symptom screen followed by smear-microscopy and targeted Xpert, contributed to improved case detection of drug-susceptible and drug-resistant TB, shortening the diagnostic delay, and successfully bringing patients into care.
Conflict of interest statement
Figures
References
-
- WHO (2013) Global Tuberculosis Report 2012. World Health Organisation, Geneva, 2012. WHO/HTM/TB/2012 6.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
